 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
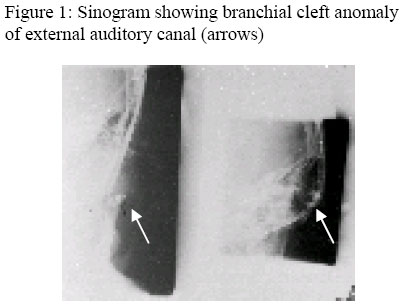
Annals of African Medicine, Vol. 2, No. 2, 2004, pp. 83-84 BRANCHIAL CLEFT ANOMALY OF EXTERNAL AUDITORY CANAL: A CASE REPORT K. R. Iseh Department of Ear, Nose and Throat, Usmanu Danfodiyo University
Teaching Hospital, Sokoto, Nigeria Code Number: am03019 ABSTRACT A 15 year old male with a first branchial cleft anomaly seen at the Usmanu Danfodiyo University Teaching Hospital Sokoto is presented. He had recurrent preauricular swelling, which was continuous with three fistulous openings in the left external auditory meatus confirmed by sinogram. It may be mistaken for chronic suppurative otitis media or lymphadenitis, hence the need for a detailed clinical assessment. Surgical excision of the tract is the treatment of choice. Key words: Branchial cleft anomaly, external auditory canal, sinogram, surgery INTRODUCTION The external auditory canal (EAC) develops from the first branchial cleft which is a groove between the mandibular and hyoid arches. The ectoderm of the first groove deepens forming a funnel shaped tube the primary meatus that eventually becomes the outer one third of the external auditory canal. 1 A solid epidermal plug extends inward forming the meatal plate which begins to resorb forming a canal. 1 Aberrations of this coordinated development can occur giving rise to duplication anomalies of the external auditory canal, stenosis or atresia. 2-3 Duplication anomalies of the external auditory canal are characterized by fistulous tracts around the external auditory canal. 2-3. They could be Type I or Type II. Type I refers to post auricular discharging sinus while Type II refers to preauricular, intracanal up to the angle of jaw, discharging sinus. 3 CASE REPORT A 15 year old male secondary school student presented with recurrent left preauricular swelling of 7 years duration. He had several repeated incisions and drainage which normally reoccur after a while. A close examination revealed 3 separate contiguous openings at the roof of the external auditory canal a bit posteriorly and at the junction of outer 1/3 and medial 2/3 of the external auditory canal. Sinogram confirmed this to be in continuity with the left preauricular mass (figure 1). He is awaiting excision of the fistulous tract. DISCUSSION Infected preauricular sinus is a common cause of preauricular swelling when the sinus opening is easily visible. Preauricular lymphadenitis is a common differential diagnosis when there is tender preauricular swelling. For this reason antibiotictherapy along with incision and drainage is the treatment usually offered. When however there is a fistulous tract lying side by side with the external auditory canal, the cycle of recurrent infection is bound to occur. Work was the first to point out this problem.2 He was able to describe some cases of recurrent discharging sinus that could only be arrested after a careful dissection of the tract. Belluci referred to this as duplication anomaly of the EAC.3 It could be mistaken for chronic suppurative otitis media. When sinogram is done and the fistulous tract confirmed, surgical excision is the treatment of choice. Thorough Medical examination backed by a high index of suspicion cannot be over emphasized in the treatment of branchial cleft defects. They pose challenges to an otorhinolaryngologist who should be prepared to handle aberrant branches of the facial nerve while carrying out any dissection.2 Physicians should take note of this unusual presentation and refer appropriately to an ear, nose and throat surgeon. It should not be treated as chronic suppurative otitis media or tuberculous adenitis. Similar cases of Branchial cleft defects have been reported from Ibadan Nigeria. 4-5 Branchial cleft anomaly of the external auditory canal is an uncommon congenital anomaly which may be confused as tuberculous lymphadenitis, or chronic suppurative otitis media. Sinogram delineates the fistulous tract. Meticulous surgical dissection avoiding branches of facial nerve is the treatment of choice. REFERENCES
Copyright 2003 - Annals of African Medicine The following images related to this document are available:Photo images[am03019f1.jpg] |
| |||||||||

{kind=link}