 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 1, 2004, pp. 22-27 RESPIRATORY SYMPTOMS AND VENTILATORY FUNCTION IMPAIRMENT AMONG WOOD WORKERS IN THE SAVANNAH BELT OF NORTHERN NIGERIA I. B. Bosan and J. U. Okpapi Department of Medicine, Ahmadu Bello University Teaching
Hospital, Zaria and Defence Industries Corporation of Nigeria (DICON) Furniture
company,
Kaduna, Nigeria Code Number: am04007 ABSTRACT Background: Exposure to wood dust and substances
connected to wood processing have been associated with a variety of health
hazzards.
Both upper and lower respiratory tract diseaes have been noticed and described.
Several publications are found in the literature on these but no such report
has come from the Savannah belt with its peculiar climatic
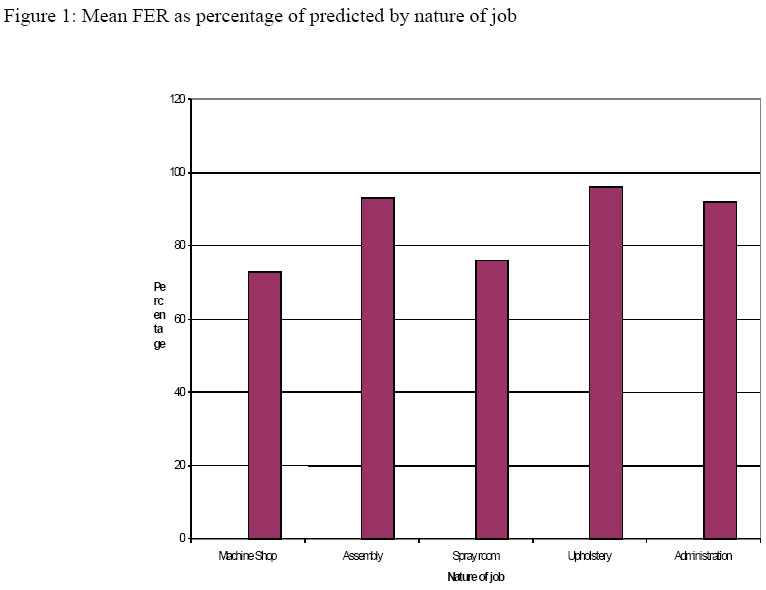
conditions. Key words: Respiratory symptoms, ventilatory function, wood furniture workers INTRODUCTION Exposure to wood dust and substances connected to wood processing have been associated with a variety of health hazards. Upper and lower respiratory diseases have been described. Among these are nasal carcinoma, 1-6 adenocarcinoma of the paranasal sinuses, 7,8 allergic rhinitis, 9,12 urticaria, 13 chronic sinusitis, 14 chronic obstructive pulmonary diseases, 15 and hypersensitivity pneumonitis. 16 Bronchial asthma has been reported associated with specific wood types. 17 - 26 Several wood industries are being established even in the non forest zones of Nigeria as a result of urbanisation, providing job opportunities for the unemployed who move from rural areas to urban centres. DICON furniture company is one of such industries situated in Kaduna, a fast developing town in the Northern part of the guinea Savannah. Kaduna is characterised by low relative humidity and two distinct wet and dry seasons. The specific objectives of this study were; 1) to determine the prevalence of respiratory symptoms and ventilatory function impairment among workers at DICON wood furniture company, 2) to determine the relationship if any, between the presence of respiratory symptoms and ventilatory function impairment, and the type, degree and duration of exposure to wood dust and/or chemicals connected to wood processing. MATERIALS AND METHODS The study was carried out during the wet months of the year to eliminate possible effect of seasonal cough, corrhiza, excessive sneezing, rhinorhoea and ocular itching that characterise the dry dusty hamattan season in this part of the country. A cross sectional descriptive study was used. The study population were all employees of the DICON furniture company. Those excluded were workers who had asthma or chronic cough before employment, those with ongoing respiratory tract infection, those on leave or absent during the period of study, and those who refused consent. The medical research council (MRC) qustionaire on respiratory symptoms modified to include smoking habits was administered for self completion. Workers who could not read and write English language, were interviewed through a common interpreter to reduce interviewer bias. Four lung function parameters; forced expiratory volume in one second (FEVI), forced vital capacity (FVC), peaked expiration flow rate (PEFR) and forced expiratory ratio (FER), which is the ratio of FEVI / FVC, were determined on all subjects using an electronic Spirometer, the micro-plus model made by Micro-medical ltd U.K. The four parameters were re-determined 15 minutes after inhalation of 200ug salbutamol aerosols using the metered dose ventolin inhaler made by Glaxo. The age, height, and weight of the subjecs were recorded. Complete blood counts and chest Xrays were done to rule out concurrent chest infection. Predicted values of FEVI, FVC, and FER for age and stature were based on formulae recommended by Patrick and Femi Pearse for the African population. 27 The predicted values of PEFR were provided by the manufacturer of the micro-plus spirometer. Although these values were based on European population which are known to be 20% higher than the African values, 27 they were valuable in analysis.nclusion. RESULTS One hunderd and fourty of the one hundred and sixty-nine employees were studied because 12 were on leave and not available for the exercise, 14 refused consent and 3 had on going chest infection. The female employees were only 6 and all of them refused consent. The 140 person studied were stratified according to their nature of job at the factory. Fourty-three (43) persons (30.7%) worked in the machine shop, their mean age was 39.5 years, mean height was 183.7cm and mean weight of 62.0kg. Thirteen (13) persons (9.3%) worked in the spray room with mean age of 42 years, mean height 167.9cm and mean weight 62.0kg. Twenty-nine (29) person (20.7%) worked at the upholstery work shop with the mean age 40 years, mean height 153.7cm and mean weight of 59.4kg. Twenty-one (21) persons (15.0%) worked in the office as administrators and support staff with mean age 38years, mean height of 166.0cm and weight of 59.6kg. There were no significant differences in mean age, height and weight between the five groups of workers (Table 1). Twenty-six (26) out of the fourty-three (43) (60.5%) (p<0.001) workers in the machine shop had respiratory symptoms of chronic cough, nasal catarrh, breathlessness and wheeze. Seven (7) out of thirteen (13) (54.9%) (p<0.001) workers in the spray room also had symptoms. However only 6 out of 34 (17.8%) of those in the assembling workshop, 6 out of 29 (20.7%) of those in the upholstery and 3 out of 21 (14.4%) of those in the administration had symptoms. Altogether 48 workers out of 140 had symptoms (34.3%) (Table 2). The presence of symptoms relative to duration of exposure among the five working groups is demonstrated in Figure 1. In the machine shop only 10% of those who had worked for less than 5 years had respiratory symptoms. After 10 years of exposure 27% had symptoms, 75% after 14 years and 93% after 19 years of exposure. A similar pattern was seen in workers in the spray room with only 10% for less than 5 years exposure, 24% after 10 years exposure 52% after 14 years exposure and 65% for those who had worked for over 19 years. There was no significant rise in the prevalence of respiratory symptoms with duration of exposure in the other groups. Twenty-seven (27) persons out of the one hundred and fourty (140) persons studied smoked cigerrette, however, there was no significant difference in the prevalence of symptoms between smokers and non smokers (Table 3). The average FEV1 (2.52 L) was lower in the smokers than the average for non smokers (2.81L) but this was not statistically significant. However, the average FVC for smokers (2.81 L) was lower than the average for non smokers (3.00L) which was significant ( p<0.05) (Table 4). The smokers were therefore excluded from further analysis of ventilatory functions to eliminate the effect of smoking on the outcome. The differences between the observed and predicted mean values of FEV1 and FVC among the workers in the machine shop were statistically significant (p<0.001). Workers in the other groups did not show significant differences (Table 5). There was no significant effect on the ventilatory functions by duration of exposure (Table 6). Forced expiratory ratio was observed to be less than 80% of the predicted values among the machine shop and spray room workers (Figure 1). There was a significant change in values of FEV1 and PEFR following the inhalation of 200ug salbutamol aerosols among workers in the machine shop and the spray room. For workers in the machine shop, the mean values of FEV1 improved from 2.52L to 2.96L (p< 0.05) and PEFR from 352 L/Min. to 441 L/min (p< 0.05). For workers in the spray room, mean values of FEV1 improved from 2.53L to 2.94L (p<0.05) and PEFR from 352L/min. to 431L/min. (p<0.05). The workers in all other working groups did not show any significant changes (Table 7). Table 1: Mean values of age, height and weight with standard error of mean, among wood workers by nature of work
Table 2: Prevalence of respiratory symptoms in wood workers by nature of work
Table 3: Prevalence of respiratory symptoms among wood workers
Table 4: Mean values of FEV1, FVC and PEFR compared with predicted values for age, sex and height among smoking and non smoking workers
NS: not significant Table 5: Mean values of FEV1 and FVC compared with predicted values for age, sex and height by the nature of work
NS: not significant Table 6: Mean values of FEV1 and FVC compared with predicted values for age, sex and height by duration of work
NS: not significant Table 7: Variation in FEV1, FVC and PEFR in wood workers following inhalation of Salbutamol aerosols by nature of work
NS: not significant DISCUSSION This study shows that respiratory symptoms such as chronic cough, corrhiza, breathlessness and wheeze were common among wood workers in the furniture construction industry in Kaduna. The prevalence of symptoms increased with increasing years of exposure. This is similar to the findings of Jinadu et al in their study among wood workers in Ile-Ife, a town in the forest zone of the country. 28 Work in the machine shop involves application of great force to model wood. This produces large quantities of respirable dusts to which the workers are exposed. The spray room workers are exposed to chemical fumes produced by the jet spraying units used to produce a forceful jet of chemicals to spray the wood. The wood dust and chemical fumes produce damaging effect on the respiratory tract through allergic reaction, direct irritant effect and/or chronic inflammatory response. The prevalence of respiratory symptoms and ventilatory impairment is highest in the machine shop and spray room workers. We believe that these groups of workers have greater exposure to respirable dust and chemical fumes than the other workers. The ambient concentration of respirable dust and chemical fumes could not be objectively measured in the present study because of the lack of appropriate facilities. However, the nature of work environment provide a fairly reliable guide to the level of exposure to these substances. Increasing prevalence of symptoms with increasing years of exposure strongly support a causal relationship. The most probable explanation is chronic inflammation from continuous exposure to the wood dust. Aging is unlikely to be a factor since there is no significant difference in mean ages among the working groups. Ventilatory function impairment appeared to get worse with increasing degree of exposure but not the duration of exposure to wood dust or chemical fumes. The most likely basis of this is allergic reaction to the wood dust and chemical fumes. The forced expiratory ratio (FER) which in the ratio of FEV1 to FVC was less than 80% of the predicted values in both the machine shop and spray room groups (Figure 2), suggesting obstructive abnormality. 29 The improvement observed after inhalation of salbutamol aerosols in the machine shop and spray room workers was greater than 15%. This meets the criteria for obstructive abnormality described by Ahuja et al. 29 Both reversible obstructive and restrictive abnormality of respiratory function have been described among wood workers. 11,29 The former described more with specific wood types. 17-26 In this study no specific wood type was evaluated. We conclude that respiratory symptoms are highly prevalent among wood workers. These are greatly influenced by the degree and duration of exposure to respirable wood dust and chemical fumes. This is probably due to both allergic reaction and non allergic chronic inflammatory response to continuous exposure. However, ventilatory function impairment which is also highly prevalent among wood workers is influenced by the degree of exposure but not the duration of exposure to wood dust and chemical fumes. The most likely basis is allergic reaction, and IgE mediated mechanism has been suggested by earlier workers. 30 We therefore recommend to all operators of woodwork industries to employ measures to reduce the degree of exposure to respirable wood dust and chemical fumes in all wood work factories. We suggest the use of appropriate breathing masks and installation of appropriate extraction belts. Finally, we suggest further studies within the west African sub-region to study the various effects of wood dust and chemicals on the physiology and immunology of wood workers. ACKNOWLEDGEMENT We acknowledge the useful advice, guidance and support of Professor C.U. Abengowe, Professor C. O. Adesanya, Dr. A. Egboga, all of the Department of medicine ABU Zaria. Also we acknowledge the contributions of Dr. A Onabolu of Haematology Department New General Hospital Kaduna, Dr (Col.) Awofeso of Radiology Department Armed Forces Reference Hospital Kaduna and Mr. O.P. Singha of community Medicine Department ABU Zaria. Our gratitude also go to Major General Adeniyi (rtd) former Director General DICON Kaduna, Alhaji M. Mubi former GM. DICON furniture Company Kaduna and the entire staff of DICON F.C. Kaduna. REFERENCES
Copyright 2004 - Annals of African Medicine The following images related to this document are available:Photo images[am04007f1.jpg] |
| |||||||||

{kind=link}