
|
Annals of African Medicine
Annals of African Medicine Society
ISSN: 1596-3519
Vol. 3, Num. 1, 2004, pp. 46-52
|
Annals of African Medicine, Vol. 3, No. 1, 2004, pp. 46-52
CONTINUING EDUCATION
PRACTICAL MANAGEMENT
OF SPINAL CORD INJURY
B. B. Shehu and N. J. Ismail
Neurosurgery Unit,
Department of Surgery, Usmanu Danfodiyo University Teaching Hospital, Sokoto,
Nigeria
Reprint requests to: Dr. B. B. Shehu, Neurosurgery Unit,
Department of Surgery, Usmanu Danfodiyo University Teaching Hospital, Sokoto,
Nigeria. E-mail: bellobalas@yahoo.co.uk
Code Number: am04014
Spinal cord injury (SCI) is a major
cause of mobility and mortality worldwide. 1,
2 Majority are caused by road traffic accidents. These patients often have
other associated injuries such as head injury, chest trauma etc. 3, 4 and
20% of patients with major spinal injury have a second spinal injury at another
level. 4, 5 The cervical spine is the most commonly affected segment
42%, followed by thoracic 31%, and lumbar 27%. 5 Mortality is higher
with spinal injury in children. Patients with incomplete injury can suffer complete
injury during transport or delay in management. Early diagnosis of injury, preservation
of spinal cord function, and maintenance or restoration of spinal alignment and
stability are the keys to successful management. The introduction of spinal cord
rehabilitation centers and the evolution of multidisciplinary trauma teams, have
led to marked improvements in the management of patients with spine and spinal
cord injuries.
BIOMECHANICS
The different mechanisms of injury
include hyperflexion, rotation, heperextension, vertical load, flexion rotation
and shearing. 5 Age, as expected affects the mechanism of injury.
In developed communities the vast majority of SCIs are caused by road traffic
accident (RTA). Fall from height (especially important in less developed countries)
and sports injury account for a considerable
proportion of SCIs. 2, 4,5 In children, birth injury, whiplash injury
and non-accidental trauma (NAT) are also important mechanisms of injury. SCIs
due to birth trauma rarely occur in vertex deliveries and are more common in
breech deliveries (67%). 6 Importantly, since most spinal birth injuries
are not accompanied by radiological abnormalities, peripheral nerve injury must
be excluded. 6, 8
PATHOPHYSIOLOGY
AND PATHOLOGY
Concussive or compressive force
to the spinal cord can lead to immediate death of
neural cell bodies in the local central gray matter. Following the initial
injury, secondary damage to the spinal cord is initiated by inflammatory response
via arachidonic acid cascade. 8, 9 There is release of excitatory
amino acids (glutamate and aspartate), and lipid peroxidation of cell membranes
by various forms of oxygen free radicals. Oedema and action of various vasoactive
inflammatory mediators, result in changes in local blood flow thereby causing
cord ischemia. There is initiation of apoptotic change in the neurons and glial
cells. 11
Trauma to the
child’s spine is more likely to result in ligamentous injury and facet capsule
rupture. In the cervical region there could be avulsion and epiphyseal separation
of basal synchondrosis of the odontoid process in the body of C2. Fracture
of the vertebral bodies and disc herniation are uncommon. There could be
a split in the cartilaginous end,
particularly the growing zone. 12, 13
Vertebral artery
injury is observed in two-third of tetraplegics who die. Depending on the severity
of trauma, contusion, infarction, laceration, transection, dural disruption,
vertebral artery injury
and total anatomic discontinuity of the cord can occur. 14
Trauma can cause spinal
epidural, intradural, or intramedulary haematoma. Localized demyelination of
damaged axons, and transsynaptic degeneration of caudal neurons lead to cord
cavitations and formation of
posttraumatic cysts.
CLASSIFICATION
Categorization is important for
treatment decision and prognosis.
-
Complete lesion: patient
with no preservation of any motor and sensory function below the level of the
injury. The chance of recovery beyond 24hours
is very little.
-
Incomplete lesion: These
are patients with residual sensory or motor function below the level of
the injury.
Types of incomplete
lesion include:
- Anterior cord syndrome
due to
damage to anterior part of the spinal cord.
- Posterior cord syndrome
due to
posterior cord damage, which is rare.
- Central cord syndrome
due to damage around the spinal canal by direct trauma, haematoma, fluid
collection or
ischemia.
- Brown-sequard syndrome 10 due
to hemi-section of the spinal cord.
- Spinal shock is a transient
loss of all neurologic function below the level of the lesion leading to
flaccid paralysis and a reflexia lasting varying period (usually 1-2 weeks). 4,
15
Some patients
suffer soft tissues injury (whiplash injury) usually following road traffic
accident. The patients complain of neck pains with or without minor neurologic
symptoms, usually the cervical x-rays
are normal. 16, 17
Some patients
suffer spinal cord injury without obvious radiologic abnormality (SCIWORA).
This type of injury commonly affects
children. 4, 18
PREHOSPITAL MANAGEMENT
The goal of management is to prevent
further injury and reduce neurological
deficits. At the site of trauma the patient is considered to have spinal injury
especially if unconscious. The cervical spine is immobilized with sand bags or
blocks. Rolled up jacket or other materials can be use to immobilize the spine.
A rigid cervical collar can be used if available. The patient is placed in supine
position if conscious or in the left lateral position with the neck immobilized
if unconscious. The airways should be protected from obstruction and inhalation
of vomitus and secretions.
Lateral bending
and rotation should be avoided. The patient should be logrolled and carried
in one piece. Hard board is used if available for transport to the hospital.
The patient is removed from the board soon after radiological evaluation
to prevent development of pressure sores.
HOSPITAL MANAGEMENT
Resuscitation
The major causes of death in a
patient with SCI are aspiration and shock. Hypoventilation and aspiration of
gastric content is common especially following high cervical injury. Initial
field or emergency room management should always begin with the basics: airway,
breathing, and circulation.
Early intubation may be
indicated when there is respiratory insufficiency. Intubation is safe when
the cervical spine is immobilized. Alternatively fiber optic intubation is
preferred when there are associated maxilofacial injuries. In the emergency
situation cricothyroidotomy, and gastric aspiration to prevent aspiration may
be required. Bradycardia, hypotension and shock can result from venous pooling,
and loss of motor and sympathetic vasomotor tone. Volume management is usually
adequate. Central catheters to assess pulmonary wedge pressure, cardiac output,
and vascular resistance are often needed. Only if effective volume resuscitation
cannot correct cardiac output should inotropic agents such as dopamine, or
neosynnephrine be used.
Immobilization
The entire spine of the patient
suspected of spinal injury should be immobilized. The following are scenarios
of suspected spinal cord injury.
Table 1: Scenarios and
evidence for suspected SCI
|
Scenario
|
Signs
|
- Major
trauma
- Ejection
from vehicle
- Hit
and run
- Holding
head in rigid position
- Apnea
following trauma
- Any
neurological deficit e.g. weakness, abdominal breathing, priapism from
autonomic dysfunction
|
- Seatbelt
bruises of neck or abdomen
- Clothes
line injury of the neck with
- Subcutaneous
emphysema
- Crepitance
or displacement of spinal process
- Vehicle
track marks across back
- Heart
rate of 80% with hypotension, consistent with spinal shock
|
The spine
should be immobilized with cervical collar and radiological evaluation carried
out to determine the level and type of
spinal injury.
The use of collar
is not practical in young children but is the standard for older children.
Laying a child younger than 7 years flat causes flexion of the cervical spine
because of the relatively large head. The trunk can be raised on folded sheets
or a hole cut out for the posterior cranium. In infants the head is best
taped to the board. The child should be removed from the board soon after radiological
evaluation to avoid pressure
necrosis of their delicate skin. 16, - 19
Evaluation
Adequate history should be taken
as soon as possible. Dragging of patient should be avoided. The patient should
be moved in one piece by the logrolling and carrying method. If a board was
used, the patient isremoved from it after radiological
evaluation. 20
Examination should
include motor functions of the major muscle groups as well as rectal examination
for sphincteric tone. Initial examination serves as a base line for subsequent
examinations.
Neurological
assessment
The adult spinal cord ends at the
lower level of L1. To determine the spinal
segment underline a given vertebra:
- The cervical nerves
1 to 8 exit
below the pedicle of their corresponding vertebra.
- For T2 to
T10 add 2 to the number of the spinous process.
- T11, T12 and
L1 over lie 11 lowest spinal segments (L1 to coccygeal
1).
- Conus medullaris lies
at L1 (in
children at L2/3). 16 - 18
Motor
level
The Royal Medical Research Council
of Great Britain scale can be used to assess muscle power (Table 2). The American
Spinal Injury Association (ASIS) motor scoring system can provide rapid assessment
(Table 3). The degree of paralysis can be assessed using the Frankel scale
(Table 4) as well as the sensory level
(Table 5).
Table 2: Royal Medical Research Council of Great Britain strength
grading scale
|
Grade
|
Strength
|
|
0
|
No contraction
|
|
1
|
Flicker or trace of contraction
|
|
2
|
Active movement with gravity eliminated
|
|
3
|
Active movement against gravity
|
|
4
|
Active movement against resistance
- 4- slight
resistance
- 4
moderate resistance
- 4+ strong
resistance
|
|
5
|
Normal strength
|
Table 3: ASIA motor
scoring system
|
Right
grade
|
Segment
|
Muscle
|
Action to test
|
Left
grade
|
|
0-5
|
C5
|
Deltoid or biceps
|
Shoulder abduction or elbow flexion
|
0-5
|
|
0-5
|
C6
|
Wrist extensors
|
Cock up wrist
|
0-5
|
|
0-5
|
C7
|
Triceps
|
Elbow extension
|
0-5
|
|
0-5
|
C8
|
Flexor digitorum profundus
|
Squeeze hand
|
0-5
|
|
0-5
|
T1
|
Hand intrinsics
|
Abduct little finger
|
0-5
|
|
0-5
|
L2
|
Iliopsoas
|
Flex hip
|
0-5
|
|
0-5
|
L3
|
Quadriceps
|
Straighten knee
|
0-5
|
|
0-5
|
L4
|
Tibialis anterior
|
Dorsiflex foot
|
0-5
|
|
0-5
|
L5
|
Extensor halllusis longus
|
Dorsiflex big toe
|
0-5
|
|
0-5
|
S1
|
Gastrocnemius
|
Plantar flex foot
|
0-5
|
|
50
|
¬ Total possible
points ®
|
50
|
|
Grand total: 100
|
Table 4: Frankel scale
|
Grade
|
Description
|
|
A or 1
|
Complete motor and sensory paralysis below the lesion
|
|
B or 2
|
Complete motor and sensory paralysis, but some residual
sensory perception below the lesion
|
|
C or 3
|
Residual motor function, but of no practical use
|
|
D or 4
|
Useful but subnormal motor function below the lesion
|
|
E or 5
|
Normal
|
Table 5: Key sensory
landmarks
|
Level
|
Dermatome
|
|
C4
|
Shoulders
|
|
C6
|
Thumb
|
|
C7
|
Middle finger
|
|
C8
|
Little finger
|
|
T4
|
Nipples
|
|
T6
|
Xiphoid
|
|
T10
|
Umbilicus
|
|
L3
|
Just above patella
|
|
L4
|
Medial malleolus
|
|
L5
|
Great toe
|
|
S1
|
Lateral malleolus
|
|
S4 - 5
|
Peri-anal
|
Investigation
Plain X-ray is indicated in all
patients with suspected spinal injury. Radiologic evaluation should be done
after adequate resuscitation and before removal of
immobilization devices.
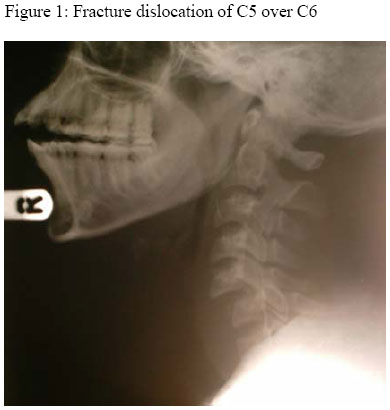
-
Cervical spine X-ray from
cranio-cervical junction to C7/T1 junction. Antero-posterior, lateral, oblique
or ‘swimmer view’ may be necessary to demonstrate lower cervical vertebrae. In
a patient with suspected odontoid process fracture open mouth view can
be carried out.
Figure 1
- Flexion-extension (dynamic)
views can be performed under medical supervision, in a patient with no neurologic
deficit that had previous normal radiograph but still having neck pains.
- Thoraco-lumbar spine X-rays:
antero-posterior and lateral view to rule out a second injury or demonstrate
fracture in cases of suspected thoraco-lumber injury.
- Computer tomography (CT)
scanning and magnetic resonance imaging (MRI) of the fractured segment
may demonstrate cord involvement or spinal canal obstruction. CT myelography
may
demonstrate
spinal block, although MRI has largely replaced it.
- Spinal angiography may demonstrate
vascular involvement especially in patients with SCIWORA.
Treatment
After resuscitation, treatment
of patients with complete injury is aimed at preventing the three major complications
of traumatic paraplegia viz pressure sore, urinary tract infection and, contracture
and deformities of the limbs. In those with incomplete injury the aim is stabilization
until spontaneous
recovery occurs.
High dose corticosteroids
(methylprednisolone), which act by limiting secondary injury, have been
found to improve functional outcome in spinal cord injuries. However data
regarding
effectiveness in children is lacking. Methylpredisolone given within
8 hours of injury has been found to have both sensory and motor benefit in
patients
with complete or incomplete spinal
cord injury. The use H2 receptor antagonist to prevent gastric
erosion by the steroid is recommended.
Prophylaxis against
deep vain thrombosis (DVT) using low dose heparin and pneumatic compression
boots is recommended after the age
of 14 years.
Skull traction
Skull traction is aimed at reducing
cervical fracture-dislocation, maintaining normal alignment, immobilizing the
spine and decompressing the spinal cord and nerve roots. It also facilitates
bone healing. It is contraindicated in:
- Atlanto-occopital dislocation.
- Type IIA or III hangman’s
fracture.
- Skull defect at anticipated
pin
site.
- In children £ 3 years.
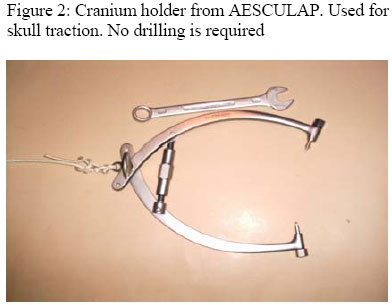
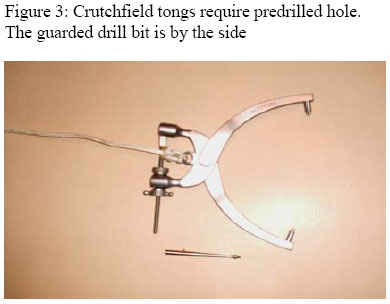
Crutchfild tongs
require pre-drilled hole. Gardner-Wells tongs or Halo ring can be used.
The pins are inserted
under local anesthesia through a stab incision above the temporalis muscle
insertion; 3 to 4 cm above the pinna, for neutral traction in line with
the external auditory meatus, 2 to 3 cm posteriorly for flexion traction
and 2
to 3 cm anteriorly for extension traction. The traction weight should
be increased gradually under radiographic
control. Formula for calculating weight:
Figure 2, Figure 3
Complication
of skull traction include:
- Skull penetration by
pins.
- Retropulsion of disc
with
neurological deterioration (need emergency CT/myelogram or MRI).
- Over distraction.
- Infections such as
osteomylitis
and subdural empyema.
Surgical management
Emergency laminectomy has been
associated with neurologic deterioration. Decompression is usually combined
with a stabilization procedure.
Incomplete
spinal injury
Patients with incomplete injury
and instability or canal compromise that do not improve on conservative management
should undergo surgical decompression and stabilization. This may facilitate
some return of neurological function.
Emergency surgery
is indicated in patients with incomplete lesion, who, following reduction of
subluxation show the following:
-
Progressive neurologic
deterioration.
- Complete spinal block on
MRI or
myelogram.
- Bone fragment within spinal
canal.
-
Cervical nerve root compression.
- Compound fracture or penetrating
spinal trauma.
- Acute anterior cord syndrome.
- Non-reducible locked facet
causing
compression.
Contraindications
to emergency operation include:
- Complete spinal cord injury
more
than 24 hours.
- Medically unfit patient.
The operative
approach could be anterior, posterior or both, depending on the mechanism of
the injury. Instrumentation (wires, cables, plates) can be used to
immobilize the area of instability while bony
fusion is occurring.
Surgical complication
include:
- Hardware problems.
- Failure of graft to take.
- Judgmental errors such as
failure
to incorporate all unstable levels.
- Postoperative kyphosis.
Complete
spinal injury
The goals of surgical management
in a patient with complete spinal lesion include:
-
Spinal stabilization before
spontaneous fusion takes place in about 8 to 12 weeks time. This
allows the patient to be placed in sitting position, improve pulmonary
function and initiate
of early rehabilitation.
-
Reduce risk of kyphotic
angulation.
Surgery should
be delayed for 4 to 5 days until the
patient is stabilized.
Bracings
Bracings are mostly used for cervical
fracture. Collars are mostly used in older children. Function is mainly to
help the patient to reduce neck movement. It immobilizes the neck very little.
The Philadelphia collar prevents neck
rotation.
Cervicothoracic
orthoses (CTO)
CTO incorporate body vest to immobilize
the cervical spine. The following have
increasing degree of immobilization.
-
Guilford brace: this is
a ring brace around the occiput and chin connected by two anterior and posterior
thoracic pads.
-
SOMI brace: acronym for
sternal occipital mandibular immobilization. Good for bracing against flexion.
Allows
patient to eat without mandibular support.
- Yale brace: An extended
Philadelphia collar. It is an effective CTO for bracing against
flexion-extension and rotation.
- Poster braces: Differ from
CTO by lack of straps under the axilla. Good for preventing
flexion at mid-cervical levels.
- Halo-vest brace: Immobilizes
upper
or lower cervical spine.
Table 6: Recommended
bracing for various cervical spine injuries
|
Condition
|
Recommended brace
|
|
Cervical strain
|
Philadelphia collar
|
|
Jefferson fracture
|
Cervicothoracic halo
|
|
Odontoid fracture
|
Cervicothoracic halo
|
|
Hangman’s fracture
|
SOMI halo
|
|
Flexion injuries
- Mid
cervical (C3-5)
- Low
cervical (C5-T1)
|
SOMI, cervicothoracic
Halo
|
|
Extension injuries
|
|
- Mid
cervical (C3-5)
- Low
cervical (C5-T1)
|
SOMI halo, cervicothoracic halo
|
Treatment of
thoracolumber spine
Table 7: The Denis three-column model has a good predictive
value
|
Column
|
Structure
|
|
Anterior
|
- Anterior
half of disc and vertebral body including anterior annulus fibrosus
- Anterior
longitudinal ligament
|
|
Middle
|
- Posterior
half of disc and vertebral body including posterior annulus fibrosus
- Posterior
longitudinal ligaments
|
|
Posterior
|
- Posterior
bony complex
- Interspinous
and supraspinous ligament, facet joints and capsule
- Ligamentum
flavum
|
Damage to more than one column
produces an unstable injury.
-
Instability of first
degree is
mainly mechanical.
-
Instability of second
degree is a
danger to neurological deficit.
-
In third degree instability
there
is associated neurologic damage.
Bed rest for 1 – 6
weeks can manage stable injury and first-degree instability. This is followed
by ambulation in an orthosis such as
thoracolumber sacral orthosis or Jewett’s brace for 3 to 5 months.
Second and
third degree instability may require thoracolumbar instrumentation. Systems
available
include:
- Harrington rods, which provide
distraction.
- Luque rods which are more
rigid
but do not provide distraction.
- Cotrel-Dubousset system
(CD
system).
Complications of
spinal cord injury
- Mortality is 4 to 10%, mostly
associated with head injury.
- Pneumonia is common with
upper
cervical injury due to aspiration.
- Urinary tract infection
from
Foley’s catheter or intermittent cauterizations.
- Ventilator dependence especially
in high cervical injury.
- Gastro intestinal ulceration.
- Constipation.
- Posttraumatic syrinx with
delayed
neurologic deterioration.
- Progressive scoliosis due
to
imbalance of muscle innervation and poor posture.
- Decubitus ulceration.
- Chronic Pain.
- Spasticity.
-
Majority of patient
with complete
injury make no improvement with or without surgery.
-
Majority of patient
with incomplete injury will make some improvement with or without,
surgery, although
some may deteriorate.
NEW TRENDS IN
THERAPY
Acute spinal cord
injury
A variety of compounds are now
being investigated which could increase spinal cord blood flow, block excitatory
amino acid receptors or modulate the immune
response. 19, 20 All these effects could improve the success of methylprednisolone.
Examples of these compounds include naloxone, aminosteroids, indomethacin and
GMI ganglioside. 21, 22
Chronic
spinal cord injury
With chronic
spinal injury the aim of therapy is to promote regeneration of functional neural
connections between the supra-spinal centers and isolated caudal segment. Several
strategies to achieve these effects are being explored. These include the effects
of growth factors (bfGF and Hnt3) on cultured neuronal cells, transplantation
of fetal nervous tissue at the site of injury and transportation of immature
oligodendrocytes. 21, 22
Another entirely new concept being investigated is that of
neuroprosthesis, but this needs further advancements in molecular biology for
any meaningful progress. 22
CONCLUSION
A systematic
and effective practical management of patients with spinal cord injury can
improve the over all outcome. A multidisciplinary approach to management can
lead to prevention of the chronic complications associated with spinal injury.
There is a need for more studies and trials to advance knowledge and outcome
of spinal cord injury.
REFERENCES
-
David P. et
al. Spinal cord injury in children. In: Principles and practice of pediatric
neurosurgery. Thieme, New
York. 1999; 955-969.
-
Badoe
E. A. A, Jaja M. O. A, Archampong E. Q (eds). Principles and practice of
surgery,
including pathology
in the tropics. University of Ghana, Accra. 2000.
-
Greenberg
M. S. Spine injuries.
In: Handbook of Neurosurgery. Thieme, New York. 2001; 686-735.
-
White
A. A. Panjabi M. M. The problem of clinical biomechanics of the spine.
Lippincott, Philadelphia. 1990;
277-378.
-
Podolsky
S. M, Baraff L. J, Simon R. R. et al. Efficacy of cervical spine immobilization
method. J Trauma 1983;
23: 687-690.
-
Bracken
M. B, Shepard M. J, Collins W. F et al. Methylprednisolone or naloxone treatment
after acute spinal cord injury: 1-year follow-up data. J Neurosurg 1992;
76:
23-31.
-
Henry
R. F, Vaccaro A. R, Mesa J. J et al. Steroids and gunshot wounds to the spine.
Neurosurgery
1997; 41:
576-584.
-
American
Spinal Injury Association: standards for neurological classification of spinal
cord
patients.
American Spinal Injury Association, Chicago. 1992.
-
Brown-Séquard
C. E. Transmission
croisée des impressions sensitives par la moelle épiniè {grave-e} re. C. R.
Séances Soc Biol Fil 1850; 2:70.
-
Green
B. A, Klose K. J, Eismont F. J. et al. Immediate management of the spinal
cord injured patient. In: Lee
B. Y, Ostrander L, Cochran V. B, Shaw W. W (eds). The spinal cord injured
patient: comprehensive management. Saunders, Philadelphia. 1991; 24-33.
-
Guttmann
L. Spinal cord injuries: comprehensive management and research. Blackwell,
Oxford. 1973.
-
Bracken
M. B, Collins W, Freeman D. F. et al. Efficacy of methylprednisolone
in acute spinal cord injury. JAMA
1984; 251:45–{endash} 52.
-
Robertson
P. Ryan M. D. Neurologic deterioration after reduction of cervical
subluxation: mechanical compression
by disc material. J Bone Joint Surg 1992; 74B: 224-227.
-
McGuire
R. A. Cervical spine arthrodesis. In: The cervical spine. The cervical spine
research society editorial
committee. Lippincott-Raven, Philadelphia. 1998; 499-508.
-
Hamilton
M. G, Myles S.T. Pediatric spinal injury: review of 174 hospital admissions.
J Neurosurg 1992; 77:
700-704.
-
Hadley
M. N, Zabramski J. M, Browner C. M, Rekate H, Sonntag V. K. H. Pediatric
spinal trauma. J Neurosurg
1988; 68: 18-24.
-
Osenbach
R. K, Menezes A. H. Pediatric spinal cord and vertebral column injury. Neurosurgery
1992; 30:
385-390.
-
Anderson
J. M, Schutt A. H. Spinal injury in children. A review of 156 cases seen
from 1950 through 1978. Mayo
Clin Proc 1980; 55:499-504.
-
Bracken
M. B, Freeman D. H, Hellenbrand K. Incidence of acute traumatic hospitalized
spinal cord injury in the United
States, 1970-1977. Am J Epidemiol 1981; 113: 615-622.
-
Ray J,
Gage F. H. Spinal cord neuroblasts proliferate in response to basic fibroblast
growth factor. J Neurosci
1994; 14:3548-3564.
-
Xu XM,
Guenard V, Kleitman N. et al. Axonal regeneration into Schwann cell-seeded
guidance channels grafted
into
transected adult rat spinal cord. J Comp Neurol 1995; 351:145-160.
-
Howland
D. R, Bregman B. S, Tessler A. et al. Transplants enhance locomotion in neonatal
kittens whose spinal cords
are transected: a behavioral and anatomical study. Exp Neurol
1995; 135:123-145.
Copyright 2004 - Annals of African Medicine
The following images related to this document are available:
Photo images
[am04014f3.jpg]
[am04014f2.jpg]
[am04014f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}