 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 2, 2004, pp. 73-76 STROKE IN SOKOTO, NIGERIA: A FIVE YEAR RETROSPECTIVE STUDY C.H. Njoku and A.B. Aduloju Department of Medicine,
Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria Code Number: am04019 ABSTRACT Background: Morbidity
and mortality from stroke is
increasing in Africa. The focus now is on prevention. Effective preventive
strategies in any locality will depend on the knowledge of the local pattern
of
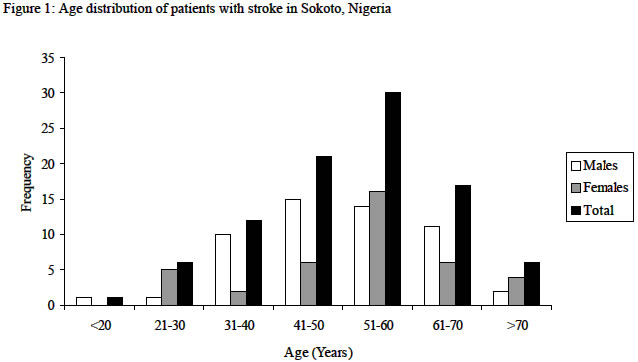
the disease. Key words: Stroke, adults, Sokoto INTRODUCTION Stroke has been defined as condition with “rapidly developing clinical signs of focal loss of cerebral function, with symptoms lasting more than 24 hours or leading to death with no apparent cause other than that of vascular origin. 1 Stroke is a global problem affecting both male and female subjects and research into this problem has been the concern of many countries. In Africa, this disease has been found to account for 0.9-4% of hospital admissions and 2.8%-4.5% of total deaths. 2 In the United States of America, it is the third leading cause of death and the leading cause of adult disability. 3,4 Case fatality rate in Africa averages about 35% but could be as low as 14.9% or as high as 77% when due to cerebral heamorrhage2. In Nigeria, stroke is a major cause of neurological admission and its incidence may be on the increase. 5,6The extended hospitalisation required in survivors with subsequent inability of many to return to work is a great burden on their family and the community. 7 The overstretched hospital personnel are equally tasked by stroke patients with their numerous demands on the limited bed spaces due to their long stay and due to their disabilities, which predispose to many complications where close care is not available. Even with intense attention and care, the outcome is not always rewarding hence prevention should be top most in our mind. As therapeutic trials are going on, guidelines for prevention are being made available. 8 Our study was therefore prompted with the latter in mind. We cannot promote prevention of the disease in our environment, if we do not know the local pattern and its peculiarities. MATERIALS AND METHOD The hospital case files of all adult stroke patients managed at Usmanu Danfodiyo University Teaching Hospital, Sokoto between the 1st of January 1994 and the 31st of December 1998 were retrieved from the medical records department and reviewed. The patients were drawn from either the casualty medical observation unit or the medical outpatient department and were subsequently admitted into the wards. The source of patient to these two outposts is usually by referral letters from peripheral hospitals or clinic or through the accident and emergency department where patients relatives could choose to bring them in the acute state without any referral letters. Each of the files was studied and all relevant data on the patients were carefully noted and recorded. These included the age of patient, sex, occupation, date of onset of illness, date of presentation, the presenting features, type of stroke (judged from clinical presentation using the WHO criteria), period of stay in the hospital, blood pressure at presentation and discharge for survivors and the out come of management of the patients. CT Scan was not done because of non-availability at the time of study. RESULTS A total of 93 patients with stroke made up of 54 males and 39 females (M: F = 2:1) were seen within the study period. These constituted 0.36% of total hospital admission at UDUTH within the same period. Sixty-eight patients (73.2%) were between 41 and 70 years, while nineteen patients (20.5%) were below 40 years. There were only six patients (6.5%) above 70 years. Majority (32.3%) of the patients were between 51 and 60 years. Twenty-one patients (22.6%) were between 41 and 50 years and 17 patients (18.3%) were between 61 and 70 years. Twelve patients (12.9%) were between 31 and 40 years. Six patients each (6.5%) were found among those between 21 and 30 years and those above 70 years. One patient was below 20 years (Figure 1). There were 38 housewives (40.9%), 20 civil servants (21.5%), 16 farmers (17.2%) and 12 business persons (12.9%). There were no records of the occupation of seven patients. Seventy-eight of the patients were hypertensive. Of the 93 patients, 42 (45.2%) had haemorrhagic stroke, 35 (37.6%) thromboembolic stroke, and 4 (4.3%) subarachnoid haemorrhage. Type of stroke was not specified in 12 (12.9%) patients (Table 1). Hemiparesis/hemiplegia was the commonest presenting feature, present in 57 patients (61.3%). Loss of consciousness was recorded in 23 patients (24.7%). Nineteen patients (20.4%) had speech impairment, which varied from sensory and motor aphasia to dysarthria. There were no of dysphonia. Other features noted were sudden collapse in 17 patients (18.3%), Headache/dizziness in 15 patients (16.1%), vomiting in ten patients (10.8%), convulsion in 4 patients (4.3%) and blurring of vision in 4 patients. Unilateral upper motor neurone facial paralysis was the only cranial nerve palsy recorded. (Table 2). Thirty-five (37.6%) of the patients died on admission. This excludes the nineteen patients, who taken away from hospital by relations against medical advice. Among the males that died, 5 (23.8%) died within twenty-four hours, 8 (38.1%) died within seven days and an additional 8 (28.1%) died between 8 to 30 days of admission. Among the females that died, 3 (21.4%) died within 24 hours, 5 (35.1%) died within seven days and additional 6 (42.9%) died between 8 and 30 days. Taken as a whole, 60% of all the deaths occurred within one week of admission (Table 3). Thirty-five patients (1.9%) died from stroke out of a total of one thousand, eight hundred and fifty six patients that died in UDUTH within the same period. Certain presenting features were noted to be associated with high mortality among the patients. These include, sudden collapse (64.7%) loss of consciousness 3.3%, headache/dizziness (53.3%) and vomiting (40%). Twelve out of twenty one patients (57.1%) aged between 41 and 50 years died. Mortality rate was 50% among those aged 21 - 30 years, 41.7% among 31 - 40 years 35.3% among those 61 to 70 years, 33.3% in those above seventy years and 23.3% in those 51 - 60 years. Eighty five percent of the deaths occurred in patients aged 31 - 70 years. Table 1: Patients distribution with respect to types of stroke
Table 2: Major presenting complaints
Table 3: Mortality at specified periods among the patients that died
DISCUSSION The stroke patients constituted 0.36% of total hospital admission within the period of study. This is lower than the 0.9 – 4.0% which has been reported from other parts of Africa. 2 Stroke is commonly regarded as a spiritual disease which demands spiritual cure rather than hospital treatment in this environment. Nineteen of our patients (20.4%) who were mainly rural farmer were withdrawn by their relatives against medical advice. This may not be unconnected with the belief. More males were affected than females in agreement with observations in other studies. 5,9,10 The male sex has been listed as a risk factor for stroke. 11 That the incidence of stroke rises with increasing age according to Osuntokun5 is supported by this study but the differential peak incidence in males in the 8th decade and females in the 7th decade was not observed in our study. The peaks occurred earlier, with the males reaching their peak incidence earlier than the females. Majority of our patients (73.2%) were between 41 and 70 years while only 6 patients (6.5%) were above 70 years. This is in agreement with findings among blacks12 and at variance with findings among Caucasians where majority of their patients are 75 years and above. 3,13 Ignorance of the risk factors for stroke and inability to control such risk factors when they are known may have contributed to this. Patients might be unknown hypertensives. Even when the patients know the risk factors, they might not believe them to be the cause of stroke nor be able to afford the cost of effective regular medication. The above reasons could have contributed in many ways to the high incidence among housewives, farmers and lowly paid civil servants. Hypertension was found to be the major risk factor to stroke among our patients. Similar findings have been noted in other studies in Nigeria. 10,14 The risk for borderline hypertension is said to be 1.5% higher than that of the Normotensive”. It has been shown that lowering blood pressure could prevent 70% of strokes. 15 We found haemorrhagic stroke to be the most common type among our patients. This agrees with the findings in some earlier studies in Nigeria16 but runs contrary to the findings in some other studies in Nigeria. 10,12,17 who found ischaemic strokes to be higher than haemorrhagic stroke. Heamorrhagic stroke is said to be higher in Asia compared to Europe and Africa. 18 Majority of those who died, died in the first week of admission. This agrees with reports of other studies. 2 The pattern of mortality seen in our study within 24 hours, seven days and thirty days agrees with the pattern seen in the aggregated data from a WHO study published in 198019. It has been stated that the high mortality rate in the first one-week may be due to raised intracranial pressure and that most deaths after one week are from preventable causes. 2 We were not able to identify these preventable causes in this study. The mortality rate of 37.6% is higher than the 14.9% - 35.0% reported for Africa2 and the developed world. 13 Osuntokun reported a mortality rate of 4-9% for Africa. 12 The 1.9% mortality recorded in relation to the total hospital admission may appear small but when viewed along the line that stroke contributed only 0.36% of total hospital admission, the burden of stroke mortality becomes more prominent. The higher mortality rate found in those with sudden collapse, headache, dizziness and loss of consciousness may not be unconnected with the fact that these may be associated with massive cerebral haemorrhage leading to raised intracranial, pressure and consequently transtentorial herniation and death. Some of these features, as well as flaccid paralysis of the patients’ arms and legs, among others have been listed as poor predictive features of immediate outcome from stroke. 20 Studies in Caucasians have shown that mortality in stroke increases with increasing years and that the risk of death in people less than 45 years is low. 9 Our findings were different; the death rate was higher in younger people instead. Stroke in our environment affects mainly those between 41 and 70 years. Research has found that 1/3 of those affected will die, 1/3 will be seriously disabled and incapable of future independent existence while one-third will make satisfactory recovery. 13 From our finding, this 2/3 that will either die or remain permanently disabled is drawn from the active segment of the community. Greater attention needs to be focussed on this group in a community setting so that the risk factors in such group could be identified. This would form the framework upon which adequate preventive measures could be put in place to save the active population from this disabling disease. ACKNOWLEDGEMENTWe acknowledge the assistance of the staff in the medical records department who diligently sorted out the case files used for this study. REFERENCES
Copyright 2004 - Annals of African Medicine The following images related to this document are available:Photo images[am04019f1.jpg] |
| |||||||||

{kind=link}