 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
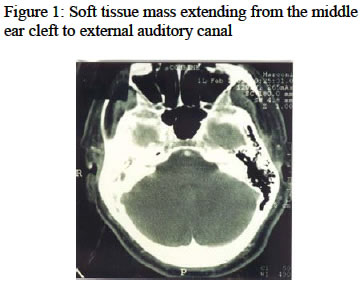
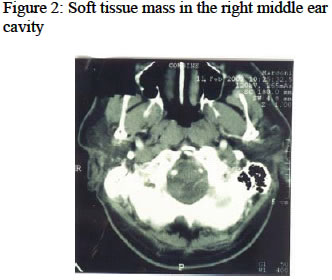
Annals of African Medicine, Vol. 3, No. 2, 2004, pp. 90-92 SQUAMOUS CELL CARCINOMA OF THE MIDDLE EAR: CASE REPORT AND LITERATURE REVIEW F. O. Agada, C. Gnananandha and M. Wickham E.
N. T. Department, Barnsley District Hospital, Barnsley, S75 2EA, United Kingdom Code Number: am04024 ABSTRACT A 50 year-old man with squamous cell carcinoma of the right middle ear is presented. Treatment was by surgery and radiotherapy. The literature is reviewed. Key words: Middle ear, carcinoma, squamous cell INTRODUCTION Middle ear squamous cell carcinoma is a rare tumour, 2 that has continued to have a dismal outcome despite increase in technology. Early diagnosis is rare2 and it is commonly associated with chronic otitis media in several reports. Case reportA 57-year-old man presented with a recent history of exacerbated discharge from the right ear. He had a history of intermittent recurrent right ear discharge for over 20 years. There has been associated difficulty in hearing but no vertigo or any neurological symptoms. Examination showed a polypoidal granular mass filling the right external auditory canal arising from the middle ear. No tympanic membrane seen. Initial histology indicated a high-grade dysplasia, suspicious of invasive malignancy. Computer tomography (CT) revealed a soft tissue mass filling the right external auditory canal, most of the right middle ear cavity, and surrounding the ossicles in the attic, which appeared intact. There was significant bony erosion adjacent to the soft tissue mass in the middle ear (Figure 1) He had exploration of the right ear, and at surgery tumour was found to extend from the external auditory canal and involving the upper mesotympanium and attic. The facial nerve was exposed in it is horizontal position 5mm. The dura was exposed and there was dehiscence of the anterior canal wall exposing the temporo -mandibular joint capsule. The stapes supra structure was not seen, however the malleus head was and embedded within the tumour. Residual tumour was left in the anterior attic over the oval window area and towards the Eustachian tube. Radical mastoidectomy and wide meatoplasty was done. Histology confirmed squamous cell carcinoma. A 6-week course of radical radiotherapy was given to the right ear. He is been followed up at the multidisciplinary joint oncology clinic. DISCUSSIONCarcinomas of the middle ear are rare tumours, it represents 5-10% of all ear neoplasm 3 and the vast majority are squamous cell carcinoma. 4The median age for these cancers is 55years, 5 however cases have been reported in children as young as 8 years.6 It is usually a unilateral disease however bilateral cases have been reported.7, 8 Chronic otitis media has been implicated as the main aetiological factor in this tumour.4, 9,10 Hence the need for a detail and regular evaluation of such patients. Radiation is the other factor implicated. More recently Jin et al11 have shown that there is a high prevalence of human papilloma virus (HPV)-16/18, at both the tissue level and molecular level, of patients with middle ear squamous cell carcinoma. This might provide an insight into the role of chronic inflammation. Middle ear squamous cell carcinoma should be considered when refractory granulation, long-standing otorrhoea, otalgia, and facial nerve palsy are observed.12 Absence of otorrhoea in the history indicates that the origin of the tumour is the external auditory canal. 4 Mastoid surgery offers no protection in the presence of continual otorrhoea.9, 10 This patient had a long-standing chronic otitis media. Diagnosis is often late; pain, facial nerve palsy and sudden deafness are often seen in the late stage of the disease.13 Therefore a high index of suspicion is necessary for an early diagnosis, especially in patients with chronic otitis media with a recent change in the pattern of their usual symptoms. This patient initially had aural polypectomy and suction clearance and initial histology was not confirmatory of squamous cell carcinoma but showed high-grade dysplasia. Confirmation of diagnosis; is by punch biopsy or subjecting the tissue removed during suction clearance to histology as in our patient. Accurate assessment of the extent of the tumour is by high resolution CT scan, 14,15 this is important in the subsequent staging and management of the tumour. Additional valuable information can be obtained from MRI were there is suspicion of vascular involvement. High resolution CT shows bone erosion and the soft tissue mass of the tumour.16 however the biological nature of the tumour is not reflected by the imaging technique. Also it is important to know that the extensive preoperative investigation often do not alter the out come of the disease but allow for proper staging and planning of treatment, even if it is palliative treatment. TNM staging allows for identification of patients who will not benefit from radical surgery thus being spared a mutilating experience, which does not add to the quality of life.17 Treatment modalities include primary surgery with a post surgical radiation in most patients; this is the preferred option.18, 19,20,21 Radiotherapy alone is considered inadequate treatment. The standard treatment for early tumour, is extended total petrosectomy with postoperative` radiotherapy, 4 however the value of such major surgery for palliation, with significant mortality and morbidity is rarely profitable in terms of cure.22 In younger patients especially with more a limited disease, a lateral or sub-total temporal resection may be considered. These procedures are not always curative, but may provide relief of the severe pain, which is so often, the most distressing aspect of the problem. Sole radiotherapy is mainly used for palliation were surgery is made impossible because of the poor general condition or in very tiny tumours.23 Our patient however had radical mastoidectomy, which was followed up by post operative radiotherapy. This is a traditional approach. Five-year survival is about 25%-50% in patients who undergo surgery and radiotherapy.23, 24 Patients with petrous bone invasion, dura invasion and distant metastasis have a gloomier outcome. Advances in technology has not improved the outcome in terms of cure. However with radiotherapy techniques becoming better, are we moving towards a lesser aggressive surgery with a better quality of life? ACKNOWLEDGEMENTS The authors wish to thank the department of medical photography and the library staff for their help. REFERENCES
Copyright 2004 - Annals of African Medicine The following images related to this document are available:Photo images[am04024f2.jpg] [am04024f1.jpg] |
| |||||||||

{kind=link}
{kind=link}