 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
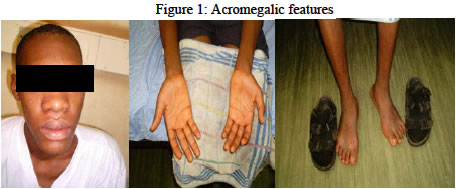
Annals of African Medicine, Vol. 3, No. 2, 2004, pp. 93-94 IMAGES IN CLINICAL PRACTICE PITUITARY MACROADENOMA B. B. Shehu, N. J. Ismail and A. O. Jimoh Neurosurgery unit, Department of Surgery, Usmanu Danfodiyo University Teaching
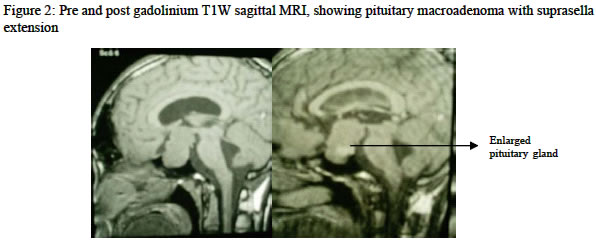
Hospital Sokoto, Nigeria Code Number: am04025 A 22 years man presented with an 8-year history of progressive enlargement of the fore head, hands and feet. He had to change his shoes frequently. Two years prior to presentation developed intermittent headache, progressive weakness, decreasing vision, slurring of speech and increase urinary frequency. The headache became severe two month before admission and associated sleep apnoea. He was found to have raised blood pressure for which he was placed on anti hypertensive drugs earlier. Physical examination showed acromegalic features (Figure 1). The blood pressure was 120/80 mmHg. There was right temporal visual field defect and vision in the left eye was reduced to finger counting at 2 meters. Magnetic resonance imaging (MRI) of the brain showed pituitary macroadenoma with suprasella extension (Figure 2). Growth hormones and prolactin levels were elevated. He was diagnosed to have acromegaly secondary to pituitary macroadenoma. His symptoms improved on oral bromocryptine 15mg 8 hourly and subcutaneous octreotide 100 µg 8 hourly. He is awaiting trans-sphenoidal resection of the pituitary macroadenoma. Excessive secretion of growth hormone (GH) in adult results in skeletal overgrowth, hypertension, soft tissue swelling and peripheral nerve entrapment syndromes, debilitating headache, palmar hyperhidrosis, oily skin, joint pain and fatigues.1 More than 95% of acromegaly cases are caused by a pituitary adenoma.2 Additionally, the mass effect of the pituitary tumor itself can cause symptoms. Compression of the optic chiasm can result in bitemporal hemianopia.1, 2 The mortality rate is at least twice that of the normal population. The major sequelae of acromegaly include cardiorespiratory and cerebrovascular diseases, diabetes, and neoplasia, particularly colon cancer.2 If the condition is present in childhood, before the closure of the epiphyses of the long bones; there is a more proportional increase in the size of all body parts, gigantism..3 Diagnosis is based on the clinical features, elevated levels of GH and IGF-I, and failure of GH suppression by glucose challenge test. Up to 20% of GH-secreting pituitary adenomas co-secrete prolactin, and the prolactin level may also be elevated.4 MRI is more sensitive in diagnosis than CT scan as it provides information about the surrounding structures. The goal of treatment is amelioration of symptoms caused by the local effects of the tumor and/or excess GH/IGF-I production. Octreotide is the most extensively studied and used somatostatin analogue.5 Medical treatment can be used before surgery to control sypmptoms and help in tumour shrinkage. This can be done with octreotide, a somastostatin analogue and bromocryptine, a dopamine agonist. Patients with residual disease can then be offered adjuvant medical treatment. Radiation treatment must be used for years to be effective.6 Trans-sphenoidal hypophysectomy has the dual advantage of rapidly improving symptoms caused by mass effect and significantly reducing or normalizing GH/IGF-I concentrations. Prognosis depends on early detection, initial size of the tumor, the GH level, presence or absence of cardiac complication and the extent of tumour resection during surgery. REFERENCES
Copyright 2004 - Annals of African Medicine The following images related to this document are available:Photo images[am04025f2.jpg] [am04025f1.jpg] |
| |||||||||

{kind=link}
{kind=link}