 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 2, 2004, pp. 95-97 Opinion EARLY DIAGNOSIS OF BREAST CANCER L. M. D. Yusufu Department of Surgery, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria ABSTRACT Cancer of the breast is the commonest malignant disease in women. It is a major public health problem worldwide. The cause is unknown, but there are documented risk factors. Most of the patients are symptomatic at the time of detection. A breast lump is by far the most common and the only symptom in majority of patients. The diagnosis is made from physical examination, imaging, cytology and biopsy. Key words: Breast cancer, early diagnosis INTRODUCTION Breast cancer is now a public health problem. 1 It is more common in women than men, in a ratio 9:1 and is one of the common malignancies diagnosed in women worldwide. 2 One of every 15 women in Europe and one of every eight women in the United State will develop breast cancer in her lifetime. 1, 3 The incidence in Nigeria is yet to be determined but ranges from 3.5% to 13.5%, in hospital based reports. 4-7 The typical pattern of breast cancer in African women consists of advanced lesions in relatively young patients, who are multiparous and have practiced prolonged lactation.8 The diagnosis of breast cancer at earlier stages is associated with a more favorable overall prognosis. 3 AETIOLOGY The cause of cancer of the breast is unknown, but there are documented risk factors. These include age; the risk is higher at 70 years than at 30 years. Previous history of breast cancer increases the risk to development of a second breast cancer by sixteen times. Nulliparity; nulliparous women have 50% increased risk. Age at first birth; women who have delivered at early age have a reduced risk. Increased parity decreases the risk for breast cancer development, although quite a large number of our patients are multiparous. 8 Artificial menopause, through bilateral oophorectomy decreases the risk of breast cancer. Breast-feeding seems to protect against pre-menopausal forms of breast cancer, the longer the breast feeding the better. 9 Obesity increases the risk at postmenopausal ages. A positive family history of breast cancer in the mother or sister increases the risk by 50% mainly in pre-menopausal age groups. Exposure to ionizing radiation around menarche increases the risk. Benign breast disease increases the risk if atypical dysplasia is present on histology. Intake of saturated fats and of total energy may increase the risk. Frequent vegetable consumption may decrease the risk.9, 10 SYMPTOMS AND SIGNS Majority of breast cancer patients are symptomatic at the time of detection and symptoms are due to local, metastatic or remote effects of the disease. A breast lump is by far the most common and the only symptom in majority of patients. Other symptoms are bloody nipple discharge, nipple abnormality and enlarged axillary lymph nodes on the same side. The most common symptoms of lump, dimpling of skin and bloody nipple discharge are however, not specific for cancer. Any woman presenting with one or more of these symptoms, should be considered to have breast cancer until proven other wise. Breast pain, which is a frequent symptom in self-referring women, is nonspecific and not, significantly associated with cancer at the early stage where there is no lump. 9,10 when it does occur the disease is probably advanced. DETECTIONThe following methods are used in detecting cancer of the breast.
BSE when regularly and properly done way detect breast cancer at an early stage. This is taught to women by medical practitioners or personnel, what appears to be a good period is just before or after menstruation. BSE should still be encouraged regularly in post-menopausal women at least monthly (Table 1). Physical examination is done by trained personnel, and is aimed also at detecting any abnormality in the breast early for further diagnostic work-up. P.E may miss cancer less than 1cm or those that are deeply located in large breasts. Mammography is accurate in cancer detection. The tumour size affects the sensitivity of M less than it does for P.E. The usefulness of M as a detection tool for breast cancer in healthy women depends mainly on age. The cutoff age most commonly advised for its use in screening is 50 years and above. In our environment cost and availability may not allow for screening at the moment. Women at risk should have M at least once every year. In its absence or non-availability, regular physical examinations should be done. Table 1: Steps for breast self-examination
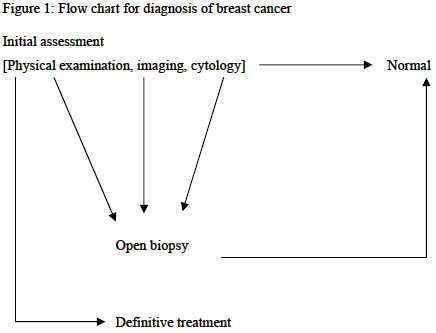
DIAGNOSIS The diagnosis of breast cancer depends on the clinical presentation. The initial assessment includes detailed clinical history, and physical examination, fine need aspiration, core biopsy, nipple discharge cytology or surgical biopsy. Mammography in selected patients. 9,11 (Figure 1). Other investigation such as sonography is also used to aid diagnostic needling of impalpable lesions and implantation of wires to guide operative biopsy. Liver function test, chest radiography, bone scans, computerized Tomographic scan are only necessary for staging the disease. I would hasten to warn against the practice of discarding surgical specimen without histological examination. This delays the patient from seeking medical attention earlier and should be condemned by all. Breast cancer is a common problem in women. The prognosis depends on the stage of presentation among others. Women should promptly seek medical advice in the presence of al breast lump, bleeding or discharge from the nipple. Specimen taken from the breast should be subjected to histological examination. REFERENCES
Copyright 2004 - Annals of African Medicine The following images related to this document are available:Photo images[am04026f1.jpg] |
| |||||||||

{kind=link}