
|
Annals of African Medicine
Annals of African Medicine Society
ISSN: 1596-3519
Vol. 3, Num. 2, 2004, pp. 95-97
|
Annals of African Medicine, Vol. 3, No. 2, 2004, pp. 98-108
CONTINUING EDUCATION
ATRIAL FIBRILLATION: CURRENT TRENDS IN MANAGEMENT
M. S. Isa, S. S. Danbauchi, M. A. Alhassan, A. I. Oyati and B. G. Sani
Department of Medicine (Cardiology Unit), Ahmadu Bello University
Teaching Hospital, Zaria, Nigeria
Reprint requests to: Dr.
M. S. ISA. E-mail: muhd_sisa@yahoo.com
Code Number: am04027
ABSTRACT
Quite a number of dramatic interventional advances in the
treatment of cardiac arrhythmias such as catheter ablation and implantable
cardiac defibrillators for serious ventricular arrhythmias have held the limelight
over the last few years. The treatment of atrial fibrillation (AF), which remains
the commonest arrhythmia affecting 0.5% of people aged 50-59 years increasing
to 12% at age above 74years, has received relatively little attention. There
is however, a recent resurgence of interest following some important experimental
and therapeutic advances. This article reviews the current understanding of
the nature of atrial fibrillation (AF) and some recent developments in the
pharmacological
and alternative therapeutic approaches.
Key words: Atrial fibrillation, treatment
INTRODUCTION
“When the pulse is irregular and
tremulous and the beats occur at intervals, then the impulse of life fades;
when the pulse is slender (smaller than feeble but still perceptible, then
like a silk thread), then the
impulse of life is small” Huang Ti Nei Ching su Wen. The atrial are far from
being a single pair of spherical surfaces with uniform electrophysiological characteristics.
They are anatomically and functionally complex structures that can provide a
substrate for various arrhythmias (atrial fibrillation inclusive), and pose a
diagnostic
and therapeutic challenge to the clinicians.
Atrial fibrillation (AF) is by far the commonest sustained cardiac arrhythmia,
with an overall prevalence of 0.5% - 1% in people
aged < 50 years, rising to about 12% in those over 74 years.1 Atrial
fibrillation, is slightly more in men than women and, the arrhythmia may either
be chronic or paroxysmal. Up to a third of patients with atrial fibrillation
may have idiopathic or “lone” atrial fibrillation, when no precipitating cause
can be identified and no evidence of structural heart
disease exists.2, 3 In most patients with chronic AF, the arrhythmia
can be attributed to organic heart disease or a metabolic disorder. Ischaemic
heart disease, coronary arterial disease, pulmonary thromboembolism, pre- excitation
syndromes are numerically more important causes of AF in the Western countries
while rheumatic heart disease, acute infections, thyrotoxicosis and hypertension
usually constitute the important causes of AF in developing
countries.3, 4 Overall, AF is associated with an increased mortality,
its presence reflecting the severity of the underlying cardiac disease, and greatly
increasing the risk of stroke.4 Non- rheumatic AF increases the risk
of stroke by a factor of five.1 This risk increases by about 5% per
year especially in the elderly, the presence of high blood pressure or other
evidence of heart disease, e.g., myocardial infarction.3,5 Table
1 shows some of the common causes of AF.
AETIOPATHOPHYSIOLOGY
Pathogenesis
The mechanism
of atrial fibrillation has recently become clearer and is understood in terms
of multiple irregular
wavelets of excitation. This understanding allows a single model to be proposed
which unites the various etiologies and treatment of atrial fibrillation (Figure
1).
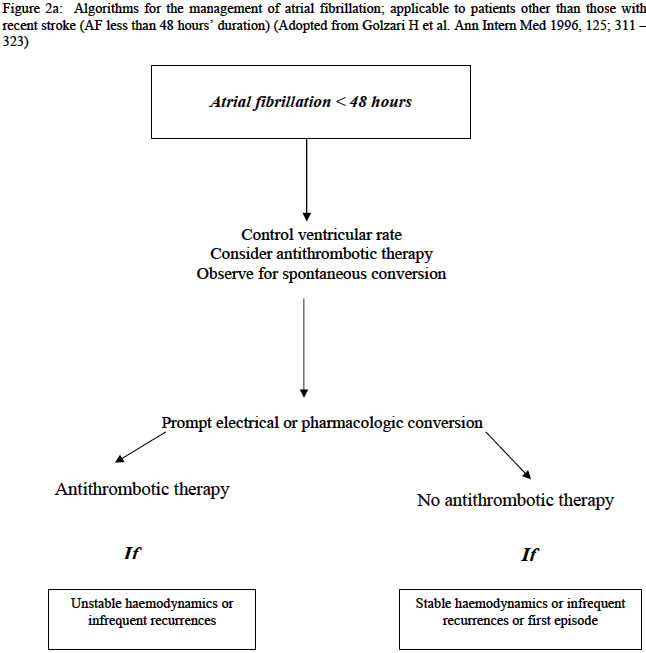
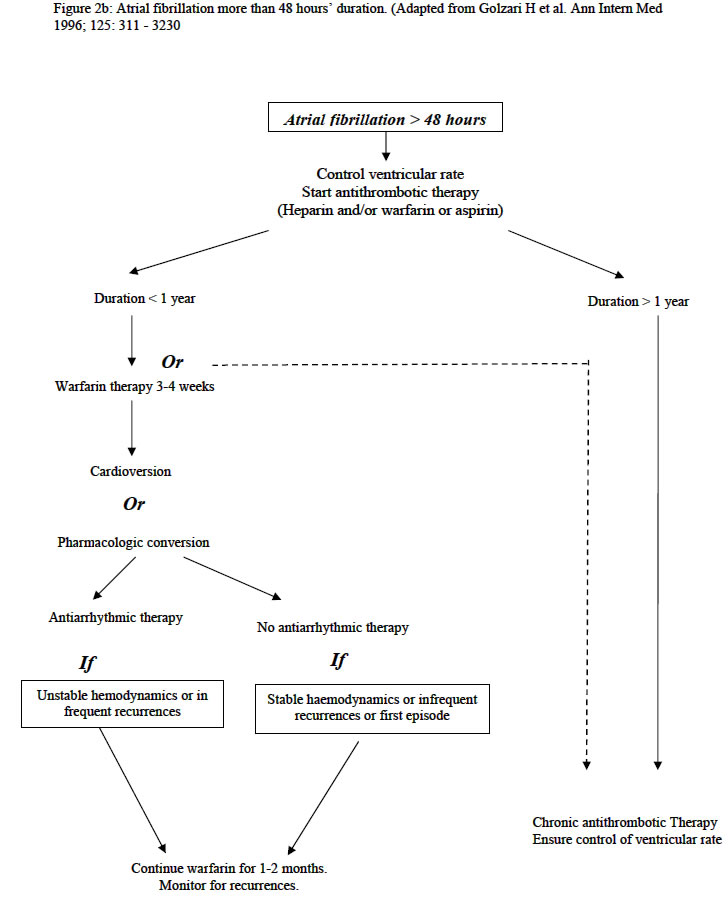
Figures 2a, 2b
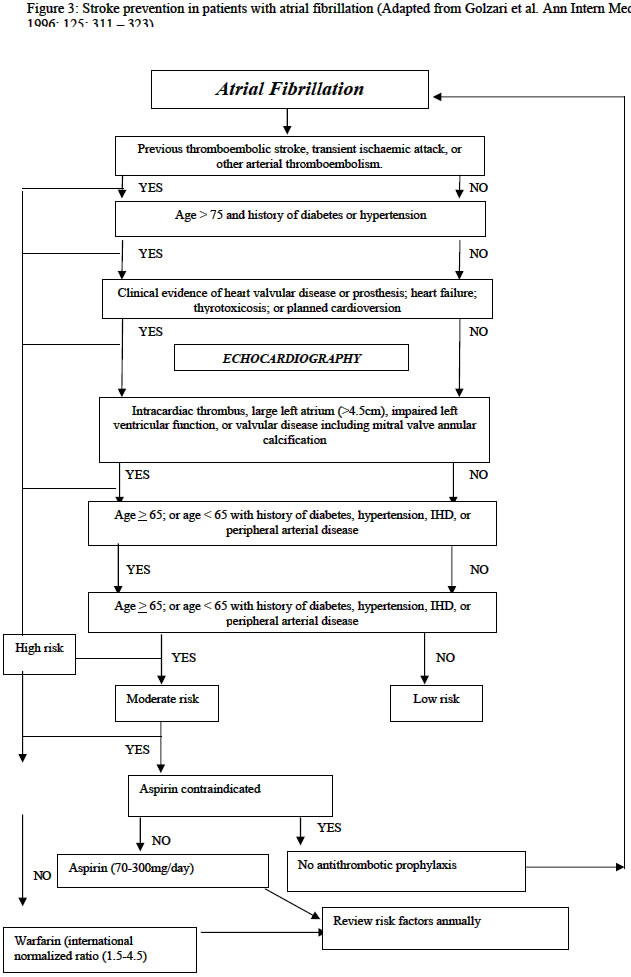
Figure 3
Cardiac arrhythmia is caused by
an abnormality in the rate regularity or site of the cardiac impulse or by
certain disturbances in the conduction of the impulse such that the normal
sequence of activation of the atria and ventricles is disturbed. This may be
explained in terms of abnormalities of impulse initiation (i.e. abnormal automaticity),
impulse conduction (re-entry) and/ or
both.6 - 12 Abnormal automaticity arises from the ability of all cardiac
tissue in the right circumstances to generate its own impulse. A rapidly firing
automatic focus can compete with the sinus node to dominate the cardiac rhythm,
e.g. tachycardia due to drug toxicity. However, re-entry occurs when the cardiac
impulse circulates in a closed loop with excitatory waves
spreading out to the rest of the heart on each
circuit, e.g., junctional tachycardia and most
ventricular tachycardias.8 Earlier experiments establish that AF cannot
arise from ectopic automatic foci, either singular or multiple, 7,8 until
Moe’s observation in 1962.7
Table 1: Some causes of
atrial fibrillation
|
Cardiac causes
|
Non – cardiac causes
|
|
Common
|
|
|
Rheumatic heart disease
|
Acute infections e.g. pneumonias
|
|
Hypertension
|
Thyrotoxicosis
|
|
Cardiomyopathy or heart muscle disease
|
Excess alcohol intake
|
|
Ischaemic heart disease
|
Pleural effusion
|
|
Pericardial disease e.g. pericarditis
|
Pulmonary thromboembolism
|
|
Sick sinus syndrome
|
Pre – excitation syndrome e.g. wpw
|
|
|
|
|
Less common
|
|
|
Atrial septal defect
|
Lung carcinoma
|
|
Atrial myxoma
|
Thoracotomy
|
In 1962, Moe proposed that AF consisted of several
co- existing re- entrant wave fronts of activation within the atria. Moe’s
model was refined and given an electrophysiological basis by experimental studies
in
the 1970s to 1990s. 7, 8, 9 These studies also showed that most wave
fronts do not in fact re- enter but rather sweep around the atria continually
invading excitable tissues and being extinguished or divide around obstacles. 10 Sustained
AF is dependent on these multiple wave fronts continually encountering excitable
tissue. This process is favored by three factors (Shortening of atrial refractoriness,
Slow conduction (allowing time for the tissue to regain excitability between
each wave front) and Increased atrial
size (and therefore surface area). 11 Mechanical stimuli (valvular,
hypertensive heart disease and failure) give rise to AF by causing atrial dilatation
and slow conduction, whereas functional factors (atria ischaemia, biochemical
abnormalities, and autonomic tone) exert various influences on conduction and
repolarisation. 10, 11
Pathophysiology
The
haemodynamic disturbance of atrial fibrillation results essentially from
the absence of atrial systole
(“atrial kick”) and from the rapidity and irregularity of the ventricular response,
with a consequent loss of cardiac output (a loss of about 10% in normal individuals
with a greater loss of ventricular rate). A rapid heart rate reduces the diastolic
filling interval, and the additional loss of the sequential atrioventricular
contraction mechanism in AF may lead to a dramatic reduction in cardiac output
and to other haemodynamic disturbances. Atrial dilatation and loss of atrial
systole leads
to intra- atrial stasis favoring the formation of thrombus.12 Also,
with the onset of a rapid ventricular rate or response, some incompetence of
the mitral valve may occur leading to further reduction of forward flow.3,
5, 12
CLINICAL SUBSETS
OF ATRIAL FIBRILLATION
For practical purposes, three distinct forms of AF according
to their pattern of occurrence are being
suggested here.3
1. Paroxysmal
atrial
fibrillation
This term is used
to describe at least one episode of self-terminating AF. The duration of the
episodes may vary from seconds to days and the interval between successive
episodes is unpredictable. The natural history of the condition is a progression
towards more prolonged episodes of AF and ultimately to persistent or permanent
AF, a process which may take many years. The goal of therapy for paroxysmal
AF is to prevent recurrences.
2. Persistent
atrial
fibrillation
This term may
be used to describe the clinical situation where an episode of AF has not spontaneously
reverted to sinus rhythm, although chemical or direct current cardioversion
is capable of restoring it. The probability of restoring sinus rhythm is dependent
on a variety of factors, in particular, duration of the episode of AF (Less
than one year) and the degree of left atrial enlargement. Usually, the probability
to restore
and maintain sinus rhythm is very low if left atrial diameter is > 6cm as
measured by echocardiography.12 In contrast, if left atrial diameter
is < 5cm, the result of cardioversion and reduction of the relapse risk by
treatment with antiarrhythmics is generally better. The patients with left atrial
diameter of 5 to 6cm generally comprise the subset with intermediate probability
for successful cardioversion.
3. Permanent
atrial
fibrillation
This term may
be used when attempts at restoration of sinus rhythm have failed or here the
probability of successful cardioversion is considered so low that no attempt
has been made. Once the permanence of AF has been determined, the objectives
of therapy become those of adequate rate
control and prophylaxis against thromboembolism.
THERAPEUTIC OPTIONS IN ATRIAL
FIBRILLATION
The therapeutic goals that should
be considered for each patient are: restoration of sinus rhythm, maintenance
of sinus rhythm, rate control and prevention of
thromboembolism.
A) Pharmacologic
methods
1. Restoration of sinus rhythm
Electrical cardioversion
is the method routinely used to restore sinus rhythm especially in haemodynamically
unstable patients.3 The best predictors of a successful cardioversion
are (Short duration of the AF, Age, Absence of underlying disease (especially
rheumatic), Heart failure (low New York Heart Association Function Class I/
II, high left ventricular
ejection fraction) and small left atria.12 However, pharmacologic
conversion of AF is often preferred and may have the particular benefit of preventing
early recurrences.13 - 16 Overall, it appears that moderate to good
efficacy in chemical cardioversion is achieved with the use of class IA, IC agents
and amiodarone 17, 18 Sotalol is less effective22 while,
digoxin, beta- blockers and calcium channel blockers (CCB) are essentially ineffective
in cardioversion, although they slow ventricular rate. 18
- 20 The use of class I anti- arrhythmic drugs to terminate AF or prevent
recurrence in acutely ill patients runs the risk of provoking serious ventricular
arrhythmia, or acute heart failure, and should therefore be
avoided.3 The efficacy of the newer class III agents such as Ibutilide
and Defetilide, appears to be very promising, but they are still awaiting clinical
use approval.15
Amiodarone is considered by some, the most effective agent for refractory,
symptomatic, recurrent AF. Although minimal prospective comparative drug data
are available, nearly two thirds of patients treated remained in sinus rhythm
for up to one year follow up.12, 21 Frequent use of amiodarone for
AF is limited due to its potentially severe and life threatening side-effects.
These however can be minimized with low daily
dosing.13 As recurrence of AF is common, successful drug therapy should
be evaluated by the decrease in number and duration of AF episodes and not its
mere recurrence. Usually, patients with long standing AF, large left atrial size,
or those with previous multiple drug failures, will experience the highest recurrence
rates.3, 12, 22, 23 In such patients, concomitant ventricular rate
control therapy with oral digoxin, verapamil, diltiazem or a beta- blocker should
be considered. 15, 20, 22 - 28
2. Maintenance of sinus rhythm
Without medical
treatment, most studies indicate persistence of sinus rhythm in only about
20-40% of patients after 1 year. 21,
29 This result can be improved by treatment with anti- arrhythmic
agents. Class IA drugs (quinidine, disopyramide, procainamide) may present some
desirable effects on electrophysiology, but accelerate atrioventricular conduction.
Quinidine has been the mainstay for AF prophylaxis, however a meta- analysis
of six placebo controlled trials 25, 30, 31 and observations from
the SPAF (Stroke Prevention in Atrial Fibrillation) trial, 26 have
shown a significantly greater mortality in patients receiving quinidine. This
has led to the reappraisal of the class IA agents in the management of
AF. By contrast, class IC drugs such as Flecainide and Propaferone, have been
well investigated.15 They have potent effects on conduction within
cardiac cell membranes and lengthen the PR interval and QRS complex in the ECG.
Flecainide has been shown to be effective in preventing recurrences of atrial
fibrillation in up to 60% of patients but does not limit the ventricular response.
Adverse effects with flecainide have been reported in up to 74% of patients,
but these effects were mostly tolerable. Nevertheless, doubts about the safety
of flecainide have been raised by the CAST (Cardiac Arrhythmia
Suppression Trial). 24 Recent studies 15, 25 however supported
the use of Propafenone and Flecainide as safe and effective choices for the pharmacological
treatment of AF, supraventricular tachycardia or premature ventricular complexes
in properly selected patients (particularly in terms of preserved left ventricular
function and without history of myocardial infarction or congestive heart failure).
In patients with recurrent episodes of AF, class IC agents are usually more effective
than class IA drugs in
maintaining sinus rhythm, and are also better tolerated. 15
The role of amiodarone
(a class III drug) inthe maintenance
of sinus rhythm is of considerable
interest. Direct comparisons suggest that
amiodarone is superior to quinidine 22, 23, 25 – 27 in efficacy and
is not responsible for an excess of deaths due to proarrhythmic effect in patients
with structural heart disease (myocardial infarction and congestive heart failure).
However, the non- cardiac side effects of amiodarone i.e. abnormal thyroid function,
lung fibrosis and corneal deposits may lead to drug in continuance. But this
can be curtailed with lower dose of 100mg/day. 28
3. Rate control in atrial
fibrillation
Pharmacological
agents that depress conduction and prolong refractoriness in the atrioventricular
node are frequently required for control of symptoms and improvement of haemodynamic
during AF. 3, 19, 26 These includes digoxin, beta- adrenergic
antagonists and calcium channel blockers.3 Optimal rate control
includes reducing resting heart rate to < 90 beats/ minute and preventing
excessive rate response on minimal exercise.14,
27
The physician attempting to slow the ventricular rate during AF must consider
two phases of treatment: an acute phase that involves rapid control of ventricular
rate and a long- term phase that involves drugs given orally to patients that
develop rapid ventricular
rates and symptomatic. 3 In the presence of important clinical symptoms,
such as chest pain or exacerbation of congestive heart failure, that are related
to a rapid ventricular response, intravenous drug therapy to slow the heart rate
relatively quickly is often required. 20 Although, intravenous digoxin
may effectively slow the ventricular rate- at rest, there is delay in its onset
of effect of at least 60 minutes in most patients, with the full effect delayed
for up to 6 hours.3, 28
Adenosine is a naturally occurring substance with a half life of approximately
10 seconds, which produces marked inhibition of AV nodal conduction. Although
it is very effective for terminating re- entrant arrhythmias using the AV node,
this agent has no role in the management of AF because of its transient duration
of action.3 For patients with severe symptoms relating to a rapid
ventricular rate, intravenous Diltiazem, Verapamil, Esmolol, Propranolol, or
Metoprolol provides
rapid control of heart rate as reported from various studies. 3, 15, 23 These
agents can result in lower heart rates during exercise than digoxin alone but
significant side effects of bradycardia and atrioventricular block should be
taken into account. This is particularly a problem in the elderly and those with
sick sinus syndrome.
Prevention
of thromboembolism
Atrial fibrillation is the most
common cardiac condition that predisposes to systemic
embolism.29 - 40 The high risks of thromboembolism stroke is the most
devastating complication commonly associated with mitral stenosis and prosthetic
mitral valves. 12, 41 - 42 AF even in the absence of any valvular
disorder, carries a substantial increase risk of ischaemic stroke especially
among the elderly, averaging about 5 percent per year. 5 But with
transient ischaemic attacks, the rate of brain ischaemia accompanying non- valvular
AF exceeds 7 percent per year.42, 43 The absolute rate of stroke varies
importantly with patient age and co- existing cardiovascular
disease 44 (Table 2).
Most ischaemic strokes associated with AF are probably due to embolism or
stasis; however, about 25 percent of AF associated stroke is due to intrinsic
cerebrovascular diseases, other cardiac sources of embolism, or aortic arch
atheroma. 35 - 41 Identification of subpopulation of AF patients
with relatively high or low absolute rates of stroke and or other risk factors
determine which patients will gain the greatest benefit from anticoagulation
therapy 39, 40, 45
Antithrombotic
therapy
Long term warfarin therapy prevent
stroke in patients who have atrial fibrillation associated with either rheumatic
valvular disease or prosthetic heart valves.46 However, in non-
rheumatic atrial fibrillation, the value of anti- coagulation therapy was not
established until the recent randomized, prospective clinical trials using
INR (International Randomize Ratio) of between 1.8- 4.2.47 Table
3. Combined analysis of these trials showed a reduction in the incidence of
ischaemic stroke or embolus from 4.5 to 1.4 percent per year for a risk reduction
of 69 percent. 46, 48
Although aspirin appeared to be beneficial in the Stroke Prevention in Atrial
Fibrillation (SPAF I) trial, 37 its efficacy relative to that of
warfarin was only established after the completion
of the SPAF II trial. 40 The study showed that the rates of ischaemic
stroke and systemic emboli for patients on 325 mg/ day of aspirin and those of
warfarin, did not differ significantly in patients 75 years or younger, in those
older than 75 years or the two groups combined. The study also confirmed that
a history of hypertension, thromboembolism or recent heart failure were important
risk factor(s) for thromboembolism.
Anticoagulation
for cardioversion
Systemic embolism is a complication
of electrical and pharmacological cardioversion of
AF to sinus rhythm.15 Prior anticoagulation appears to decrease the
embolic risk, 47 even though no randomized, controlled prospective
trials evaluating the efficacy of prophylactic anticoagulation therapies in this
setting have been performed. Current recommendations are to give anticoagulants
to patients who have AF of unknown duration or more than 48 hours for approximately
3 weeks before and 4 weeks after cardioversion. 15 Alternatively,
TEE (Transaesophageal Echocardiography) has been suggested as another approach
for in hospital patients with AF lasting more than 2 days. 46,
48 The role of immediate anticoagulation therapy for atrial fibrillation
of less than 48 hours duration remains unexplored. 27
Anticoagulation therapy is substantially more effective than aspirin in the
secondary prevention of stroke and vascular
events. 41 The European Atrial Fibrillation Trial, 47 showed
a 47 percent reduction in the overall risk for vascular events and a decrease
in the rate of stroke from 12 to 4 percent per year. However, optimal time for
initiating anticoagulation therapy in patients with recent onset stroke and atrial
fibrillation is still controversial. The Cerebral Embolism
Study Group, 48 proposed that, in patients with a small or moderate
infarction, anticoagulation therapy should be initiated if no evidence of hemorrhage
is shown on CT scan 24 to 48 hours after the stroke. In patients who have a large
infarction, anticoagulation therapy should be started if after 7 days, CT excludes
the possibility of delayed hemorrhage.
Table 2: Factors associated with high risk of stroke in patients
with AF
|
Age > 65 years
|
|
Hypertension
|
|
Rheumatic heart disease
|
|
Prior stroke or transient ischaemia attacks (TIA)
|
|
Diabetes mellitus
|
|
Congestive heart failure
|
|
Left atrial dimension > 5 cm
|
Table 3: Recommendation(s) for long term anticoagulation in
patients with chronic atrial fibrillation
|
Age (years)
|
Risk factors
|
Recommendations
|
|
< 65
|
Absent
|
Aspirin
|
|
|
Present
|
Warfarin (target inr 2.5)
|
|
65 - 75
|
Absent
|
Aspirin or warfarin
|
|
|
Present
|
Warfarin (target inr 2.5)
|
|
> 75
|
All present
|
Warfarin (target inr 2.5)
|
Risks factors: Prior transient ischaemic attack, systemic
embolus, or stroke, hypertension, poor left ventricular function, rheumatic
mitral valve disease, prosthetic heart valve Adapted from: A laupacis et al:
chest 114: 579s, 1998.
B) Non-
pharmacologic therapies
A
variety of non – pharmacological techniques are being developed for use as alternatives
and /or adjuncts to drug therapy. These include:
1. Atrial pacing
The realization
that episodes of AF often occur at times of sinus bradycardia or following
sinus pauses, suggests that atrial pacing may have a preventive role in the
treatment of AF.3 Overdrive suppression is a common technique in
the acute management of atrial and ventricular arrhythmias but has not been
subjected to trials in long – term
use.3, 12 However, there is preliminary evidence that dual chamber
pacing at a rate slightly higher than the mean sinus rate, reduces the incidence
of atrial arrhythmias. 3
2. Atrioventricular nodal ablation
The established
treatment for AF that is refractory to pharmacological therapy is ablation
of the atrioventricular (AV) node. This was originally undertaken using ligation
or cryo – surgery via right atriotomy, but that method has been supplanted
in the last decade by catheter based
techniques. 14, 49 - 53
3. Direct current radiofrequency
energy 50 delivered to a catheter tip positioned adjacent to the
AV node can be reliably used to produce complete AV block. Furthermore, the
procedure is generally painless and thus, can be done without general anesthesia.
AV nodal ablation is not a cure for AF, it simply disconnects the ventricles
from the atria and the sinus node and therefore, the patient will require a
permanent ventricular pace maker. Although such patients no longer suffer symptoms
due to an irregular or rapid pulse, atrial transport is not regained nor is
the risk of thromboembolism lessened. Thus, the ideal candidate for this procedure
is an elderly patient in whom paced cardiac rhythm is an acceptable alternative
to chronic, expensive and often ineffective pharmacological therapy with frequent
hospital attendance.51
C) Surgery
for atrial fibrillation
A variety of surgical procedures
have been developed for the treatment of refractory paroxysmal or chronic
AF. These aim at restoring a regular ventricular rhythm driven by the sinus
node
and hence retain a normal rate response to exercise. The two most promising
are: the “corridor” and “maze” procedures. The corridor procedure effectively
isolates both the left and right atria, leaving a strip of myocardium connecting
the sinus node to the AV. 52 This procedure does not prevent AF,
but the AV node and hence the ventricles,
are not affected by the AF.
The most radical operation devised the maze procedure, aims to completely
prevent AF. 52, 53 A series of incisions divides the entire atrium
into a labyrinth, the passages of which allow all parts to be excited by impulses
arriving from the sino- atrial node but are of insufficient width to allow
reentry. This is the only surgical procedure that restores coordinated atrial
as well as ventricular electrical activity. 3 The relative merits
of the corridor and maze procedures remain theoretical but should become clearer
with increasing experience. Surgery is likely to remain an unusual treatment
for AF, being reserved for younger patients with severe and refractory symptom
who do not wish to be committed to life long artificial
cardiac pacing.
CONCLUSION
AF in all forms is a common and
challenging arrhythmia. The long term treatment cannot be defined after first
consultation and the approach therefore, needs to
be flexible. The “sinus rhythm restoration and maintenance” strategy whenever
it is possible, is a better option than “good ventricular rate control” strategy.
In general, prophylaxis against thromboembolism should be initiated at the first
diagnosis of AF not be discontinued until stable sinus rhythm has been documented
over a period of months. Class IC agents have demonstrated an overall better
efficacy and fewer side- effects than class IA agents in properly selected patients,
while amiodarone is especially effective in preventing AF on a short term basis.
For cases that are refractory to conventional therapy, catheter ablation and
pacemaker based and surgical treatments are becoming available, but their long
term outcomes are unknown.
REFERENCES
-
Lip GYH, Beevers DG. History,
epidemiology and importance of atrial fibrillation. BMJ 1995; 311: 1361-1363.
-
Sopher SM, Camm AJ. Atrial
fibrillation: maintenance of sinus rhythm versus rate control. Am J Cardiol
1996; 77: 24A-37A.
-
Roberts J, Kloosterman EM,
Castellanus A. Recognition, clinical assessment and management of arrhythmias
and conduction disturbances. In: Fuster V, Alexander RW, O’Rourke RA, Roberts
R, King III SB, Wellens HJJ (Eds). Hurst’s: the heart. McGraw – Hill, New York.
2001; 797 – 873.
-
Wolf PA, Abbott R, Kannel
WB. Atrial fibrillation as an independent risk factor for stroke. The Framingham
study. Stroke 1991; 22: 983- 988.
-
Murgatroyd FD, Camm AJ.
Current
concepts in atrial fibrillation. Br J Hosp Med 1993; 48: 546-560.
-
Allessie MA, Konings K,
Kirchhof CJHJ, Wijffels M. Electrophysiologic mechanisms of perpetuation
of atrial
fibrillation. Am J Cardiol 1996; 77: 10A - 23A.
-
Moe GK. On the multiple
wavelet hypothesis of atrial fibrillation. Arch Int Pharmacodyn Ther 1962;
140:
183-188.
-
Allessie MA, Bonke FIM,
Schopman
FIG.Circus movements
in rabbit atrial muscle as a
mechanism of tachycardia III. The “leading circle” concept: a new model of
circus movement in cardiac tissue without the involvement of an anatomical
obstacle.
Circ Res 1977; 41: 9-10
-
Allessie MA, Brugada J,
Boersma I et al. Mapping of atrial fibrillation in man (abstract). Eur Heart
J 1990;
11(suppl) 5.
-
Sanfillippo AJ, Abascal VMM, Shecham M et
al. Atrial enlargement as a consequence of atrial fibrillation. A prospective
echocardiographic study. Circulation 1990; 82: 792.18.
-
Jane MJ. Why does atrial fibrillation occur?
Eur Heart J 1997; 18 (Suppl C): 12C – 18C. Pritchett ELC. Management
of atrial fibrillation. N Engl J Med 1992, 326: 1264-1271.
-
Miller JM, Zipes DP. Management of patients
with cardiac arrhythmias. In: Braunwald E, Zipes DP, Libby P (Eds). Heart
Disease: a textbook of cardiovascular medicine. Saunders, Philadelphia.
2001; 700 – 774.
-
Roy D et al. Amiodarone to prevent recurrence
of atrial fibrillation. Canadian trial of atrial fibrillation investigators.
N Engl J Med 2000; 342: 913-920.
-
Van Gelder IC, Crijjins HJ, Van Gilst WH,
Vermer R, Lie KI. Production of uneventful cardioversion and maintenance of
sinus rhythm from direct current electrical cardioversion of chronic atrial
fibrillation and flutter. Am J Cardiol 1991; 68: 41-46.
-
Kingman JH, Suttrop MJ. Acute pharmacologic
conversion of atrial fibrillation and flutter: The role of flecainide, propafenone
and verapamil. Am J Cardiol 1992; 7: 50A- 60A.
-
Lip GYH, Watson RDS, Singh SP. Drugs for
atrial fibrillation. BMJ 1995; 311: 1631-1634.
-
Coumel P, Thomas O, Leenhardt A. Drug therapy
for prevention of atrial fibrillation. Am J Cardiol 1996; 77: 3A-
9A.
-
Josephson ME, Zimetbaum P. The tachyarrhythmias.
In: Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL (Eds).
Harrison’s principles of internal medicine, McGraw – Hill, New York. 2001;
1292 – 1308.
-
Cobbe SM. Using the right: A treatment algorithms
for atrial fibrillation. Eur Heart J 1997; 18(Suppl C):
C33-C40.
-
Smith TW. Digitalis: mechanisms of action
and clinical use. N Engl J Med 1988; 318: 358-365.
-
Rawles JM. What is meant by a “controlled” ventricular
rate? Br Heart J 1990; 63: 157-161.
-
Coplen SE, Autmann EM, Berlin JA, Newitt
P, Chalmers TC. Efficacy and safety of quinidine therapy for maintenance of
sinus rhythm after cardioversion. Circulation 1990; 82: 1106-1116.
-
Flacker GC, Blackshear JL, McBride R, Kronmal
RA, Halperin JL. On behalf of stroke prevention in atrial fibrillation investigators.
Antiarrhythmic drug therapy and cardiac mortality in atrial fibrillation. J
Am Coll Cardiol 1992; 20: 527- 537.
-
Ruskin JN. The cardiac arrhythmia suppression
trial (CAST). N Engl J Med 1989; 321: 386- 388.
-
Lau CP, Leung WH, Wong CK. A randomized double-
blind cross – over study comparing the efficacy and tolerance of flecainide
and quinidine in the control of patients with symptomatic paroxysmal
atrial fibrillation. Am Heart J 1992; 124: 645-650.
-
Olgin JE, Zipes DP. Specific arrhythmias:
diagnosis and treatment. In: Braunwald E, Zipes DP, Libby P (Eds). Heart
Disease: A textbook of cardiovascular medicine. Saunders, Philadelphia.
2001; 815 – 889.
-
Golzari H, Cebul PD, Bahler R. Atrial fibrillation:
restoration and maintenance of sinus rhythm and indication for anticoagulation
therapy. Ann Intern Med 1996; 125: 311- 323.
-
Reiter MJ, Shand DG, Aanonsen LM, Wagener
R, McCarthy E, Pritchett EL. Pharmacokinetics of verapamil: experience with
a sustained intravenous infusion regimen. Am J Cardiol 1992; 50: 716- 721.
-
Lip GYH, Lowe GDO. Anti- thrombotic treatment
for atrial fibrillation. BMJ 1995; 312: 45- 49.
-
Morley J, Marinchak R, Rials SJ, Kawey P.
Atrial fibrillation anticoagulation and stroke. Am J Cardiol 1996; 77: 38A-
39A.
-
Caro JJ, Groome PA, Flegel KM. Atrial fibrillation
and anticoagulation from randomized trials to practice. Lancet 1993; 341: 1381-
1384.
-
Clarke- Grahame C, Swanton RH. Anticoagulation
trials. Br J Hosp Med 1996; 56: 25-28.
-
Hayes CV. Randomized trials of warfarin for
atrial fibrillation. N Engl J Med 1992; 327: 1451-1460.
-
Autmann EM. Maintaining sinus rhythm with
anti- fibrillatory drugs in atrial fibrillation. Am J Cardiol 1996; 78 (suppl
4): 67-72.
-
Risk factors for stroke and efficacy of antithrombotic
therapy in atrial fibrillation. Analysis of pooled data from five randomized
controlled trials. Arch Intern Med 1994; 154:
1449-1457.
-
Peterson P, Boysen G, Godtfredsen J, Andersen
ED, Andersen B. Placebo- controlled, randomized trial of warfarin and Aspirin
for prevention of thromboembolic complication in chronic atrial fibrillation
(AFASAK). Lancet 1989; 1: 175-179.
-
Stroke prevention in atrial fibrillation
study (SPAF I), final results. Circulation 1991; 84: 527-539
-
The effect of low- dose warfarin on the risk
of stroke in patients with non- rheumatic atrial fibrillation. The Boston area
anticoagulation trial for atrial fibrillation investigation (BAATAF). N Engl
J Med 1990; 323: 1505-1511.
-
Ezekowitz MD, Bridges SL, James KE et al.
Warfarin in the prevention of stroke associated with non- rheumatic atrial
fibrillation veteran affairs; Stroke prevention in non- rheumaticatrial fibrillation
investigators (SPINAF). N Engl J
Med 1992; 327: 1406-1412.
-
Warfarin versus aspirin for prevention of
thromboembolism in atrial fibrillation; Stroke prevention in atrial fibrillation
II study (SPAF II). Lancet 1994; 343: 687-691.
-
Connelly SJ, Laupacis A, Gent M, Roberts
RS, Cairns JA, Joyner C. Canadian atrial fibrillation anticoagulation (CAFA)
study. J Am Coll Cardiol 1991; 18: 349-355.
-
Miller VT, Rothrock JF, Pearce LA, Feinberg
WM, Hart RG, Andersen DC. Ischaemic stroke in patients with atrial fibrillation;
effect of Aspirin according to stroke mechanism: Stroke prevention in atrial
fibrillation investigation. Neurology 1993; 43: 36-46.
-
Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation,
a major contributor to stroke in the elderly: The Framingham study. Arch Intern
Med 1987; 147: 1561-1564.
-
Miller VT, Pearce LA, Feinberg WM, Rothrock
JF, Andersen DC, Hart RG. For the stroke prevention in atrial fibrillation
investigators. Differential effect of aspirin versus warfarin on clinical stroke
types in patients with atrial fibrillation. Neurology 1996; 46:
238-240.
-
Prevention of stroke in atrial fibrillation.
N Engl J Med 1990; 323: 484-494.
-
Manning WJ, Silverman DI, Keighley CS, Oettgen
P, Douglas PS. Transaesophageal echocardiography facilitated early cardioversion
from atrial fibrillation using short term anticoagulation: Final results of
a prospective 45 years study. J Am Coll Cardiol 1995; 25: 1354-1361.
-
The European atrial fibrillation trial study
group. Optimal oral anticoagulation therapy in patients with non- rheumatic
atrial fibrillation and recent cerebral ischaemia. N Engl J Med 1995; 333:
5-10.
-
Cardioembolic stroke, early anticoagulation
and brain hemorrhage. Cerebral embolism study group. Arch Intern Med 1987;
147: 636-740.
-
Ferguson TB (Jr). Surgery for atrial fibrillation.
Coronary Artery Dis 1995; 6: 120-125.
-
Huang DT et al. Hybrid pharmacologic and
ablative therapy: a novel and effective approach for the management of atrial
fibrillation. J Cardiovasc Electrophysiol 1998; 9:
462-470.
-
Gallagher JJ, Svensen RH, Kassell JH et al.
Catheter technique for closed chest ablation of the atrioventricular conduction
system: a therapeutic alternative for the treatment of refractory supraventricular
tachycardia. N Engl J Med 1982; 306: 194-200.
-
Cox JL, Schuessler RB, D’Agostino HJJ et
al. The surgical treatment of atrial fibrillation III: Development of
definitive surgical procedure. J Thorac Cardiovasc Surg 1991B; 101: 569-583.
-
McComb JM. Surgery for atrial fibrillation
(Editorial). Br Heart J 1994; 71: 501-505.
Copyright 2004 - Annals of African Medicine
The following images related to this document are available:
Photo images
[am04027f2b.jpg]
[am04027f3.jpg]
[am04027f2a.jpg]
[am04027f1.gif]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}