 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 3, 2004, pp. 153-158 TRADITIONAL CATARACT TREATMENT AND THE HEALERS PERSPECTIVE: DIALOGUE WITH WESTERN SCIENCE AND TECHNOLOGY IN NIGERIA, WEST AFRICA W. E. Schrader Leiden Ethnosystems and Development program
(LEAD), Leiden University, Institute of Cultural and Social Studies, Department
of Medical Anthropology and Etnobotany, Pieter de la Court Building, Wassenaarseweg
52, Leiden, The Netherlands Code Number: am04039 ABSTRACT Background: Approximately
18 million people are blind from cataract in developing countries and this
number tends to double every 20 to 25 years. Cataract is curable by a simple
surgical procedure. The surgical output is not keeping pace with the growing
needs. In rural Sub Saharan-Africa, Morocco, India, Nepal and China, blinding
cataract is still frequently treated by traditional techniques of couching,
a locally available treatment at affordable costs. Couching is a dislocation
of the lens by a sharp artefact or by blunt manipulation. According to some
retrospective studies, couching can result in blindness due to rupture of
the lens capsule. Complete loss of sight with 50% of the patients treated
is reported. Other authors reported better results in prospective studies
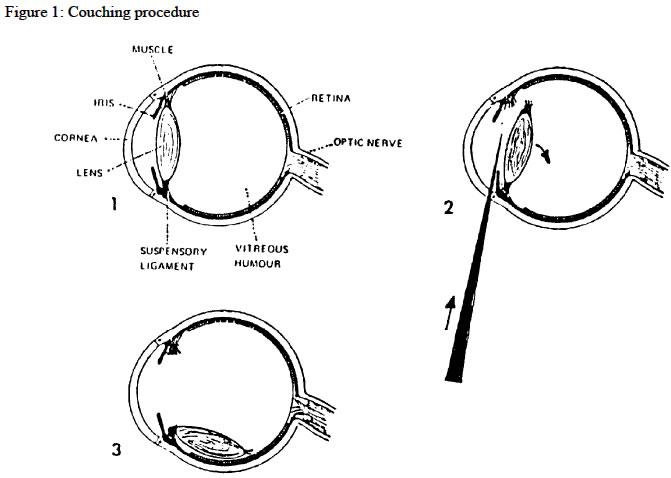
and in clinical settings. Key words: Cataract, traditional medicine, couching, community health INTRODUCTION In the magic year 2000 an estimated 38-42 million people were suffering from blindness (vision less than 3/60 in the better eye). A further 110 million people suffer from low vision and are at risk of becoming blind. The estimated world-wide prevalence of blindness is 0.7%, ranging from 0.3% in the Western world to 1.4% in Sub-Saharan Africa. 1 According to the WHO there are approximately 16-18 million people blind from cataract in developing countries and this number tends to double every 20 to 25 years. Cataract is curable by a relatively simple but delicate surgical procedure. The yearly number of operated patients, the surgical output, is however not keeping pace with the growing needs. 2 For example India has made impressive strides in building up staffing and infrastructure for the control of cataract blindness, in the period between 1990-1996.These efforts have resulted in an increase in cataract surgery from 1.1 million operations to approximately 2.2 million cataract operations year since 1994 (sometimes 2 operations are performed on 1 patient and not every operation is successful in restoring sight). Unfortunately, in India at the moment yearly 2.5 to 5.8 million sight restoring operations are required, so subsequently cataract blindness in India has increased further during the last decade. 3 Demographic changes like population growth and ageing are the main reasons for the increase in cataract blindness. It seems logistically rather impossible to restore vision in this huge number of individuals by modern standard eye surgical procedures. 4 - 6 As a consequence, world-wide approximately 85% of patients blind from cataract go untreated. In rural Sub Saharan-Africa, 7 - 13 Morocco, 3, 14 India, 15, 16 Nepal 17, 18 and China, 19 however, blinding cataract in recent history and still now often is treated by traditional techniques of couching, a locally available treatment at a cost that members of a rural community can afford. This traditional treatment is a mechanical dislocation of the lens usually by a sharp artefact (Figure 1) or by blunt manipulation. The technique of couching, the traditional treatment for cataract, goes back to the Assyrian Code of King Hammurabi around 1700 BC, 20 and the Hindu surgeon Susruta around 700 BC. 21 For the Greek, the Romans as well as Egyptians, 22 Arabs 23, 24 and Europeans 25 couching was the only choice for treatment for more than three thousand years until the late 19th century. However, according to ophthalmologists, supported by retrospective studies, 3, 15, 17, 18, 26, 27 couching can result in rupture of the lens capsule producing endophthalmitis, uveitis, and glaucoma. Most of these publications report a complete loss of sight with 50% of the treated patients. For example, Brandt et al 18 examined 100 eyes that had undergone couching by "quacks" one to 10 years earlier. At the time of the examination, 42 eyes were found to be blind, most of the blindness occurred immediately after the operation or within six months. However, an important finding was that 58% of the eyes had vision preserved for the first year, and subsequent yearly loss of vision was less than 10%. Belyaev and Barachkov 28 reported on 68 eyes that were couched in a clinical setting and followed for more than 5 years. Vision of 20/20 to 20/40 was obtained in 56 of 68 (82%). In 26 eyes without other pathologic lesions, vision was 20/20. Eyes with other previous pathologic conditions, such as corneal opacification or glaucoma, had a mean visual acuity of 20/50 as a result. There were only three complications, one a ruptured capsule requiring extraction and two with vitreous prolapse into the anterior chamber, producing glaucoma that required a vitrectomy. Despite the many complications that may occur from couching (as a result of rupture of the lens capsule), the practice continues in various parts of the world, particularly in China, India, Nepal and Africa. Traditional couchers, observed as being dominantly male, and almost exclusively trained by their fathers, continue to perform this ancient technique especially in rural areas, both as established healers in specific communities, as well as travelling around like other professional groups in the population, due to their trade. Although this practice is still dismissed by many if not most Western ophthalmologists, the authors review of ten key articles on the subject shows that in research projects with a prospective approach these traditional techniques provide surprisingly good results. By the authors of these articles, couching is regarded as a promising appropriate alternative for the Western technique of lens-extraction. In the 1990’s two ophthalmologists, Girard 29 and Worst 30 proposed that the dislocation of the cataractous lens could be performed by a modified technique of couching. They proposed lens relocation with the use of a frozen probe and zonulolytic agents like Alphachymotrypsin. With this technique the lens capsule and anterior vitreous hyaloid would remain intact. When the entire lens, including the capsule is displaced, the technique is well tolerated and will hardly cause inflammation or glaucoma, lens capsule ruptures, anterior vitreous loss or lens displacement into the anterior chamber causing pupillary block. When the anterior vitreous hyaloid is left intact, these complications do not seem to occur. Girard 29 reported a pilot study in which 82% of the eyes treated with Alphachymotrypsin showed lens displacement and an intact anterior vitreous hyaloid after a year of observation. Patients without pre-existing ocular pathology had their vision easily corrected with spectacles once their lens was dislocated with this technique. A lens, which has been dislocated downwards and has not been damaged usually is well tolerated for years and is compatible with good vision. 31 In rural Nigeria, in places where there is hardly any access to modern eye-surgery, according to the healers, an estimated 10.000 cataract blind people are being treated yearly with rather good results, by a so far unknown herbal therapy. In the 1990’s the herbalists had obtained the approval of the health authorities to perform their treatment. The herbalists claim that their ancient herbal method of couching can easily compete with the western method of lens-extraction. As a matter of fact they regard the invasive western method as dangerous and inferior to their non-invasive technique. MATERIALS AND METHODS This retrospective study took place in Wura Hausa, a small community of approximately 12,000 inhabitants near Yola, Adamawa State, in the southern part of north eastern Nigeria, during a ten-day period in December 1994. The data were collected in co-operation with the traditional healers themselves. Consecutive patients of a traditional eye centre who had been treated for cataract by couching were interviewed and examined. Examination of the patients ranged from history taking, registration of the method of treatment, name of the healer, sex, age and parameters of socio-economic status, such as occupation, literacy and education as well as visual function and mobility before and after treatment. (ADL-scale). Furthermore an inspection of the ocular adnexa, conjunctivae, sclerae, and anterior chamber took place during the study. In addition determination of best visual acuity with and without correction using the Snellen E chart and fundus examination by direct ophthalmoscopy was performed. Intraocular pressure was estimated by palpation. The study included 48 patients, 22 women and 26 men, ranging in age from 30-90 years. The average age was 68 years (SD 13). According to the histories taken, all 65 eyes treated had been blind before treatment. The 48 patients had undergone treatment of one or both eyes by a traditional method from 5 minutes to 15 years previously (average 3.2 years). Three patients were observed both pre- and post-treatment. The treatment technique, according to the herbal practitioners and patients interviewed, consisted of topical application of a liquid herbal preparation to the eye. Excluded from the study were those aphakic patients that had been treated surgically at a specialized Western eye hospital nearby or who showed evidence of previously performed intraocular surgical procedures. RESULTS Forty-two (65%) of the 65 eyes examined showed a corrected visual acuity between 20/20 and 20/40 (Table 1). Sixteen eyes (25%) showed a corrected visual acuity between 20/40 and 20/200. The median refractive correction for optimal vision was + 10.0 D (range -2.00 to + 13.00 D). There was neither observed evidence of an invasive technique having been performed nor evidence of infectious consequences. Ophthalmoscopic examination showed the cataractous lens to be displaced downwards in the treated eyes. The remaining seven eyes (10%) showed a corrected visual acuity of less than 20/200. In these eyes, vision loss was related to previous or concomitant pathology, i.e., corneal scarring in three eyes, glaucoma in two eyes and undetermined in two eyes (Table 2). In the three eyes that were observed before and immediately after treatment, the pre-treatment visual acuity was <20/400. Prior to treatment 33 patients (79%) required a caretaker. Following treatments there were only four patients that required a caretaker, in three cases due to old age. Table 1: Spherically corrected visual acuities of 65 eyes in 48 patients undergoing cataract displacement by traditional herbal topical preparation
Source: Visual field work survey Table 2: Causes for visual acuity <20/200 in 7 eyes with displaced cataracts
The author made the observations of the 65 eyes that had undergone local treatment of couching which resulted in dislocation of the cataractous lens with the assistance of a traditional herbalist. The treatment was described to the observer by the traditional herbalists and by all patients examined. These conditions can possibly cause bias such as positive patient selection and selective presentation of information. The research group was not a randomised selection from the consecutive group of treated patients. All interviews were video-recorded to be interpreted afterwards. This treatment, as described by those interviewed, was painless but caused an itching sensation. The patients were told to open their eyes while the practitioner examined them to determine if instillation of additional drops was necessary. The patients were told not to sleep in the afternoon, and stand upright as much as possible for three days following the treatment. The traditional practitioners and the patients both said that there was no penetration of the cornea or sclera by any instrument. Also, the author observed no evidence of an incision or any other invasive procedure. According to two Nigerian traditional eye practitioners, Alahadji and his son Mohammed Abdulahi Nasidi, the indication for a non-invasive displacement of the lens is the obvious presence of a mature cataract. They were able to make the distinction that a lens displacement technique is not advisable for immature cataracts, but is preferable performed in mature cataracts, as shown in the following statements: Alahadji Abdulahi Nasidi stated: "We encounter different types of cataracts. Most are pure and white - these are the best to work on. A bright green cataract is difficult to work on and there are brown and golden cataracts which will need a long treatment with many medicines to cure it." Mohammed Abdulahi Nasidi stated: "We close the eye and open it. If it (the pupil) closes and opens and the cataract will come out and show, we can work on it. The calabash and the cataract can be compared. If the calabash is too young and you cut it, it will rot and you can never use it again. But if it is ripe, you can cut it and you can use it and no water will be spoiled. If a patient can see the moon or fire in the night, yet not see other things, we can work on him and we are sure he will see perfectly well, but if he doesn't see it (the moon in the night), we will reject the patient, because the eye is already dead." These statements indicate that the traditional healers do exactly know that a pupillary reaction to a light stimulus indicates an intact retina and optic nerve pathway. Furthermore they differentiated six types of cataract, all with a different therapeutic approach and prognosis. The striking feature in their description is that their categorisation of cataract and their distinctions between the various types of treatment refers to classifications that are also found in tenth century Arabic 23, 24 and sixteenth century European ophthalmic literature. 25 This may indicate that the knowledge was transferred by different ways of transmission through history and culture, across continents and across regional boundaries. Also other investigators have observed the successful displacement of cataractous lenses by traditional herbalists with variable results. Mariotti and Amza examined 26 eyes in 22 patients that had been treated by topical herbal preparations. 9 They observed six eyes that had complete displacement of the lens into the vitreous without rupture of the lens capsule. These eyes showed no signs of inflammation. In four eyes the vision was correctable to 20/20 with a spherical correction. Ntim-Amponsah 8 mentioned the use of an herbal preparation as well. DISCUSSION Every cataract patient, wherever in the world has the right to receive the best treatment available, which is the modern phaco-emulsification with lens implantation. However, since it is logistically impossible to cure the 18 million blind from cataract in developing countries with this modern technique, alternative methods which are presently being used, should be thoroughly examined. An alternative method to displace the cataractous lens from the optical pathway that is safe and inexpensive could contribute to solving the problem of world-wide cataract. A modern couching procedure like the injection of a zonulolytic enzyme, 29 may be a promising technique. However, an agent that will penetrate the cornea without causing damage to this structure should be used preferably, but has not been developed up until now. The traditional herbalists claim to have a solution to this problem. Displacement of the cataractous lens as practised in couching proves to restore vision to those blind from cataract in developing countries. Depending on the technique applied and the skills of the traditional Healer it appears that it has the potential to be a rapid, simple, locally available, inexpensive and safe procedure, and possibly one that can be administered by non-medical personnel. Those who can afford modern surgical techniques and the implantation of intraocular lenses will probably prefer to utilise this option. However, this option is not available to most people in rural area. If the traditional herbalists of Africa have found a zonulolytic agent that will penetrate the cornea and displace the lens without causing damage to the cornea or adjacent structures, wide scale application of these techniques is feasible, and can help solving the growing cataract problem. According to the traditional herbalists, the herbal eye drops are relatively inexpensive and easy to prepare. Implications The Nigerian Organisation of Traditional Herbalists has participated in research programmes and strives for integration into Community Health Care development. This recent change in attitude among members of the most influential organisation of Nigerian traditional herbalists in their meeting with representatives of western medicine opens new possibilities for mutual stimulation and encouragement of research programmes. 32 Among the main questions is how these healers can make their therapies more generally available while protecting their local knowledge and livelihood. In March 1996 the above-mentioned Nigerian healers, i.e. the Nasidi family were involved in an agreement with the intention of formalising the contact between the indigenous healers and a Western party interested in curing blindness on a larger scale with alternative methods. The dialog between the traditional healers and the Western trained scientist resulted in a statement drawn up by a legal counsellor, Murtala Aminu & Co., on behalf of the Nasidi family, in which the objectives of such a formal contract were listed as follows: i. To perform within the confines of traditional restrictions and sensibilities of Nasidi family, a study on the effects and complications of traditional treatment of Cataract. ii. To further develop and implement a non-invasive traditional treatment for mature Cataract. iii. To produce and issue optimal aphakic Spectacles to patients after treatment. iv. To establish factories for production of medicated Soap, Eye-drops and other Herbal products with the goal of assisting those suffering and treated for Cataract eye defects. v. To establish a Botanical Garden and herbal farm at Yola. It seems very appropriate that almost simultaneously, a project proposal was submitted by a member of the formal health community in Nigeria, expressing the need to integrate the traditional diagnosis and treatment to supplement the lack in official health care resources in the treatment of blindness. 33 In this particular proposal, the objectives from the perspective of the Ministry of Health are formulated as follows: i. Increase the surgical treatment output for cataract in Adamawa state. At present this is not keeping pace with an increasing backlog of Cataract patients and should increase significantly. ii. Increase and integrate Preventive Eye Care, which in this part of West Africa is of great necessity. Several Governmental and Non-Governmental Organizations who lack adequate resources to cover the State and specifically their target populations are providing this service. With the addition of minimal funds and improved coordination the prevalence of blinding afflictions will be reduced. Both these documents give an idea of the atmosphere in which parties that are both very much familiar with the current health situation in rural areas, express the common desire to find a way of extending the delivery of services. One of the most striking features in these documents, in our view, is that the family clearly lists the contribution they feel they can make to the medical field, but does not omit to include the related economic reciprocity. Irrespective of how the intentions focus on eye-treatment, this should also be seen as a phenomenon in which the medical knowledge and the application thereof is never isolated from the personal circumstances of the owner of either the knowledge or the resources to apply it. Motives for the exchange of knowledge regarding the traditional treatment seem to be present and are necessary for the integration into an already formalised health care delivery system. Exchange for the sake of sharing knowledge does not seem to be a priority. In the contract with the Traditional Healers the role of the intermediary agent is stated as to: i. "Collate information on effectiveness and complications, if any, between the conventional western-style hospital treatment and the application of the traditional herbal cure for cataract". ii. "The project will protect the rights of the intellectual property through patent application". These statements were taken from the March 1996 document presented by the Legal Representative of the Nasidi family as mentioned above. The value of these statements for this research is the fact that they are incorporated into a legal contract while simultaneously the Nigerian Ministry of Health has paved the way for further research within a regional development programme: According to the project proposal from the Ministry of Health 33 involvement of the health officials is included. "In co-operation with the Nigerian health authorities, a design is made for comparative research" Another important factor is the fact that for production of low-cost therapies, the organisation of herbalists relies largely on sustainable, non-destructive exploitation of forest resources. To compensate for rapid deforestation and environmental changes, the organisation is seeking assistance to start herbal plantations. In addition, attention is asked for the position of local healers and their medicinal plants in the context of indigenous property rights. Considering positive results of similar initiatives, but also problems that may emerge, 34 future research should be conducted in cooperation with traditional healers working in the area. Technology to strengthen their claims should be made available. Further research within an effective collaborative programme is recommended. REFERENCES
Copyright 2004 - Annals of African Medicine The following images related to this document are available:Photo images[am04039f1.jpg] |
| |||||||||

{kind=link}