 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 3, 2004, pp. 159-160 IMAGES IN CLINICAL PRACTICE CRANIOPHARYNGIOMA B. B. Shehu, N. J. Ismail and A. O. Jimoh Neurosurgery unit, Department of Surgery, Usmanu
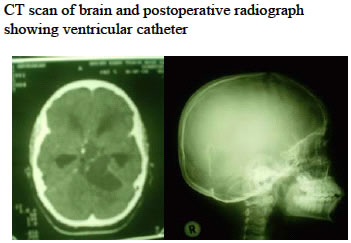
Danfodiyo University Teaching Hospital Sokoto, Nigeria. A 13-year-old boy presented with a 3-year history of occasional generalized headache, later becoming persistent and associated with early morning vomiting. He noticed progressive blurring of vision, dizziness and difficulty with walking (unable to walk beyond 10 metres) 6 months prior to presentation. The child is shorter than his two other brothers and he is over weight. There was no history of trauma and no excessive passage of urine. Physical examination showed an obese and short child (Figure 1) with bilateral papiloedema. The pulse rate was 80 per minutes, blood pressure 110/70 mmHg and the respiratory rate 20 cycles per minute. The Glasgow Coma Score (GCS) was 15 and there were signs of left cerebella dysfunction. There were exaggerated deep tendon reflexes and up going planter response. Brain computed tomography scan showed a cystic supra-sellar mass extending to the left cerebello-pontine angle with cyst wall calcification. There was enlargement of the lateral ventricles and periventricular hypodencity (Figure 2). A diagnosis of craniopharyingioma with secondary hydrocephalus was made. The pack cell volume was 35%, white blood cell count 4.0 ´ 109/ L and serum electrolytes and urea were normal. A ventricular catheter connected to a subgalial reservoir was inserted into the cystic potion of the tumour (Figure 2) via a left posterior fossa craniotomy. Twenty millilitres of brownish fluid was drained. A further 3mls of the fluid was drained 10 days postoperatively. The child improved and was able to walk, the headache subsided and vision improved. A repeat fundoscopy 3 weeks postoperatively showed pale right disc with normal vessels while the left disc margin was slightly obscure with reduced venous pulsation. Craniotomy and excision of the tumour is planned. Craniopharyngiomas constitute about 3% of all intracranial neoplasms. 1 They are the most common paediatric brain tumour of nonglial origin. Half of all cases occur in adults. 2, 3 The tumour grows from epithelial rests derived from the Rathke cleft, which is the embryonal precursor to the adenohypophysis. Despite the benign histology, their intimate association with visual apparatus, hypothalamus and the ventricular system frequently predisposes the patient to visual impairment, endocrine dysfunction and hydrocephalus. 4 Almost 93% of children have signs of growth failure, whereas the majority of adults develop sexual or menstrual dysfunction. 5 Obesity, which is frequently present could be due to pressure to the ventromedial area (the so-called ‘satiety centre), leading to hyperphagia, 5 but may also be observed after damage to catecholaminergic pathways traversing the area. Computed tomography and magnetic resonance imaging are the investigations of choice. Hydrocephalus is present preoperatively in 15 to 30 per cent of patients with craniopharyngioma, and this complicating factor must be dealt with before definitive tumour therapy is attempted. 6 In this patient the drainage of the cystic potion of the tumour helped to re-establish the cerebrospinal fluid pathways. Shunting procedure could also be carried out. Tumour resection is best accomplished via subfrontal or trans-sphenoidally for intra sellar tumours. Total tumour removal offers the best chance of cure. Adhesion to surrounding brain tissue or blood vessels can result in subtotal resection and higher incidence of recurrence. Radiation therapy (and intracystic chemotherapy in some paediatric patients) may control residual or recurrent tumour. 7 REFERENCES
Copyright 2004 - Annals of African Medicine The following images related to this document are available:Photo images[am04040f1.jpg] [am04040f2.jpg] |
| |||||||||

{kind=link}
{kind=link}