 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 4, 2004, pp. 164-166 PATTERN AND BACTERIOLOGY OF ACUTE SUPPURATIVE OTITIS MEDIA IN SOKOTO, NIGERIA K. R. Iseh and T. Adegbite Department of Ear, Nose and Throat, UsmanuDanfodiyoUniversity
Teaching Hospital, Sokoto, Nigeria Code Number: am04042 Abstract Background:To describe the pattern of distribution,
causative bacterial organisms, and management of acute suppurative otitis media
in Sokoto, Nigeria. Key words: Acute suppurative otitis media, Staphylococcus aureus
Introduction
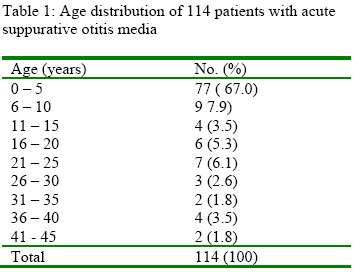
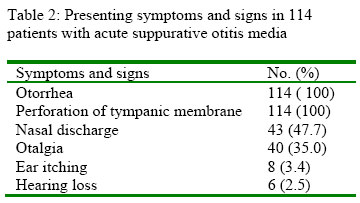
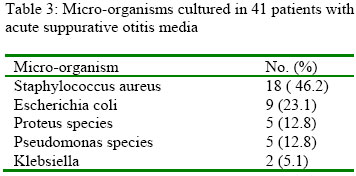
The inflammation of the middle ear cleft known as otitis media could be acute, subacute or chronic. 1-4 The acute form if not recognized early is commonly characterized by suppuration from the middle ear following perforation of the tympanic membrane. It is the commonest ear pathology in otorhinolaryngological practice. It is also the commonest paediatric otorhinolaryngological presentation. Otalgia followed by otorhoea are the commonest symptoms prior to presentation in the hospital. Many predisposing factors have been reported in the literature, such as age, (commoner in younger children) cold climatic conditions, race, upper respiratory tract infection, immune deficiency states, malnutrition, tumours of the nose and nasopharynx.1-4.In this report, the pattern of distribution and causative bacterial organisms of acute suppurative otitis media (ASOM) in Sokoto, Nigeria. Patients and Methods Clinical records of patients with ear discharge of less than 3 weeks duration diagnosed as acute suppurative otitis media at first presentation were reviewed for age, sex, clinical presentation, bacteriology and management from January, 1998 to December, 1999, in the Ear, Nose and Throat Department of Usmanu Danfodiyo University Teaching Hospital (UDUTH) Sokoto. Bacteriology and antibiotic sensitivity tests were carried out in the microbiology department of the same Hospital. There were no facilities for isolation of anaerobic bacteria or fungi. Results A total number of 114 case folders were accessible out of the 219 patients diagnosed during the period for acute suppurative otitis media. There were 70 males (61.4%) and 44 females (38.6%) with a male to female ratio of 1.6:1. The age range of presentation was between 17 days and 45 years, with 0-5 years accounting for 67.5% as shown in table 1. The commonest presenting symptoms and signs were otorrhea and tympanic membrane perforation (100%), nasal discharge (47.7%) and otalgia (35.0%), as shown in table 2. Ear swab was cultured in only 41 patients (36%). Staphylococcus aureus (46.2%) was the commonest bacteria cultured followed by Escherichia coli (23.1%) as shown in table 3.
Discussion
Acute suppurative otitis media is a common disease in children. In this report, 0-5 years age group accounted for 67.5%. This is similar to other reports.1-5.Children are more prone due to a number of reasons such as susceptibility to upper respiratory tract infections, more horizontal nature of Eustachian tubes, and immaturity of immune system. 1-5. Otorrhoea was the commonest presenting symptom followed by otalgia. It is the ear discharge due to tympanic membrane perforation that brings patients to the hospital. Tympanic membrane perforation and suppuration may be arrested if excessive crying with touching of the ear is detected early and confirmed by otoscopic examination. This usually reveals hyperaemic tympanic membrane. Prompt antibiotic and nasal decongestant treatment will abort suppuration. Staphylococcus aureus was the commonest micro-organism cultured. It has also been cultured in other reports in Nigeria. 7-8 This is a beta-lactamase producing bacteria. The implication is that treatment with antibiotics that are active against beta-lactamase producing bacteria will be more effective in preventing progression from ASOM to the chronic chronic suppurative otitis media (CSOM). However Brobby in Ghana cultured streptococcus pyogenes in patients who had suppuration within 7 days. 9 Subsequent discharges were secondarily contaminated and cultured other micro-organisms and it was suggested that penicillin was still effective. But quite a large number still progressed to the chronic stage as penicillin was ineffective. Our pattern of bacteriology is different from those reported in western literature where Streptococcus pneumoniae, Haemophilus influenzae and Moraxella (Branhamella) catarrhalis are widely reported from the United States of America, Canada, Colombia, Finland, Sweden and Japan as the leading bacteria pathogens followed by streptococcus Group A and Staphylococcus aureus. 1-6 Some European studies found Haemophilus influenzae to be the most common organism followed by streptococcus pneumoniae and Branhamella catarrhalis. 1-6 There was mastoiditis as a complication in one of the patients. This is a well-known complication of otitis media. 2-4. The low incidence of mastoiditis in this study may be due to widespread antibiotic self medicationin Nigeria before seeking treatment in hospital. Failure of resolution of acute suppurative otitis media with persistent ear discharge will lead to a chronically discharging ear, cronic suppurative otitis media (CSOM) .1-5,10 It is suggested therefore that antibiotics active against beta- lactamase producing bacteria other than penicillins may offer a better option in treating ASOM in Nigeria. Penicillins which are widely used are inactive against beta-lactamase producing bacteria. This may be the reason amongst others for progression to chronic suppurative otitis media when only penicillins are used. Augmentin (Amoxicillin +Clavulanate potassium) an antibiotic active against beta-lactamase producing bacteria, though more expensive, was used in some of our patients . A trial so far on 30 consecutive patients with ASOM showed reduction and cessation of ear discharge within 5 days. The course of treatment was however for 10 days along with oral antihistamine (chlorpheniramine). Daily aural toileting was carried out until there was no more discharge. Further trials with other antibiotics active against beta lactamase producing bacteria are necessary to compare results in terms of cost effectiveness in the treatment of ASOM in a developing countries like Nigeria. This will reduce the rate of progression to CSOM which is a more complex condition to manage. References
Copyright 2004 - Annals of African Medicine |

{kind=link}
{kind=link}
{kind=link}