 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 4, 2004, pp. 167-169 CLINICAL DIAGNOSIS OF STROKE: NEED FOR AUDIT I. Imam and G. Olorunfemi Department of Medicine, Gwagwalada Specialist
Hospital, Abuja, Nigeria Code Number: am04043 Abstract Background: Stroke is a common disease and in developing
countries its diagnosis relies heavily on clinical features because of the
dearth of radiological facilities. To ensure that the diagnosis of stroke is as
accurate as possible, it is imperative that clinical skills are kept at the
optimum. One such method of doing this is by clinical audit. This study looked
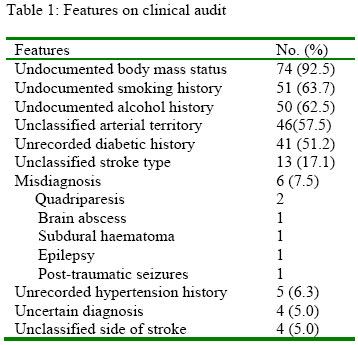
at the clinical diagnosis of stroke in a retrospective review of case notes. Key words: Stroke, diagnosis, audit Introduction Stroke is a common and devastating disease that has a poorer prognosis in blacks. 1-3 Accurate diagnosis of stroke site, size and type requires radiological tests because errors occur with clinical methods. 4, 5 In most parts of Africa however, radiological tests like computerised tomography (CT) scans are unavailable or expensive with the implication that a vast majority of stroke diagnoses in Africa rely solely on clinical methods. Because of this, there is a need to subject these methods to periodic audit in order to improve the outcome in management of stroke cases. We present one such audit in a tertiary hospital setting where CT scan facilities are not available and we also give an overview of steps to an accurate stroke diagnosis. Method The case records of all patients admitted into the medical wards of a 300-bed specialist’s hospital in Gwagwalada, within Nigeria’s Federal Capital Territory. The cases were admitted over a five-year period covering 1996 to 2000. The criteria accepted for diagnosis of stroke were sudden onset of a focal or global neurological deficit lasting more than 24 hours or leading to death for which there are no other obvious causes. We recorded details of history and clinical examination used to diagnose and classify stroke. Results Eighty-six case records were reviewed. Six did not fulfil the criteria for diagnosis of stroke and the history and findings strongly suggested alternative diagnoses which were subdural haematoma, epilepsy, post traumatic seizures, brain abscess and two cases of quadriparesis of uncertain cause. Four cases were excluded on the basis of conflicting findings on documentation. Seventy-six case records were accepted as fulfilling the criteria for diagnosis of stroke. There were 47 males (61.8%) and 29 females (38.2%). The mean age was 52.9 years with a range of 20-80. Sixty-two cases (81.6%) could be classified as thrombotic, haemorrhagic or embolic but data was insufficient to classify 13 cases (17.1%). The side of the stroke was classified in 72 cases (94.7%) but in 4 cases (5.3%) the side of stroke was not recorded. These were cases in which the subjects were deeply unconscious however. Arterial territory involvement was not identified in 46 cases (61.3%). A history of pre-existing hypertension was not recorded in 5 cases (6.6%). Previous diabetic status was also not established in 41 cases (53.9%). Alcohol history was not documented in 50 subjects (65.7%). Smoking history was not documented in 51 subjects (67.1%) (Table 1). HIV and body mass status were referred to in only two subjects each. Discussion The rate of obvious stroke misdiagnoses in this study is 7.5%. This would be higher if CT scans were done in the subjects as clinical criteria in Nigerians have been shown to misdiagnose 13 to 43% of patients. 6, 7 This emphasises the fact that even without CT scans, stroke misdiagnoses could be avoided if clinical signs are interpreted correctly. The necessity of this is underscored by the fact that most misdiagnosed stroke cases are remediable such as subdural haematomas and brain abscesses. 2, 6-8 This is demonstrated by the 6 cases that were misdiagnosed in this study. Data in the cases studied was insufficient to properly classify stroke in 18.4% and approaches previous reports of 21% stroke misclassification. 4, 5 This figure would however be higher if CT scans were done. The therapy of stroke depends on stroke type and the need to classify stroke types cannot be underestimated. 9 Various clinical scales have been evolved to improve the diagnosis and classification of stroke. 10, 11 The Siriraj and Guy’s Hospitals scores for example have been validated for clinical diagnosis and even for commencing thrombolytic therapy. 12, 13 Though this is contentious, it has been established that failure to seek and interpret clinical symptoms and signs are responsible for the most stroke misdiagnoses. 6 It has also been recognised however that CT scans are invaluable in the early identification of surgically remediable conditions often misdiagnosed as stroke. 7 The main features used for stroke classification are the typical temporal profile, stroke settings and symptoms. Haemorrhagic intracerebral bleeds usually occur on activity, may progress over minutes, and are more likely to be associated with decreased level of consciousness, vomiting, headache and severe hypertension. Subarachnoid haemorrhages are particularly associated with the most severe headaches, worse impairment of consciousness, nuchal rigidity, subhyaloid haemorrhages and a bloody cerebrospinal fluid tap. Thrombotic strokes usually occur after a period of inactivity and may follow a slowly progressive course. The findings of artheroma markers like carotid bruits and locomotor brachialis are highly suggestive of thrombotic strokes. Embolic strokes are the most sudden, may occur on activity, have maximum disability at onset and progressively improve thereafter. Finding cardiac arrhythmias are suggestive of embolic strokes. This study has shown that in most cases, emphasis is not placed on identification of the arterial territory involved in stroke; it was not recorded in 57.6% of the cases assessed. It is however of diagnostic significance in subjects with recurrent strokes. Involvement of the same territory would suggest a thrombotic stroke while involvement of different territories may suggest cardio-embolic embolic strokes. It is also of prognostic significance as posterior circulation strokes have a worse outcome. History of pre-existing hypertension was the only stroke risk factor that was consistently recorded in the case records assessed in this study. This is justified by the fact that hypertension is the most important stroke risk factor and the most amenable to control. 2, 14-16 There is however the need to assess all other risk factors so as to make secondary prevention possible. The most common risk factors apart from hypertension are diabetes mellitus, atrial fibrillation, transient ischaemic attacks, prior stroke, alcoholism and smoking. 17 The significance of HIV infection as a risk factor for stroke in Africans is unclear as studies give conflicting findings. 18,19 With the increasing incidence of HIV infections however, there may be a need to record HIV status in all stroke subjects because it may present with amenable stroke-like conditions like tuberculomas, brain abscesses and central nervous system toxoplasmosis. This audit has emphasised the need to utilise all clinical tools to diagnose and classify stroke as well as to address all risk factors. There is however the need to make CT scans widely available and affordable, as this is the most reliable means of diagnosis and classification of stroke8. With the right orientation, many African governments can make CT scans more available to aid stroke diagnosis and management. Early CT scans can detect haemorrhages which appear as enhancing lesions. Thrombolytic and antithrombotic therapy may be commenced in the absence of CT evidence of haemorrhage but this may convert ischaemic lesions to haemorrhagic ones. CT scans also have a role in establishing stroke data banks which improve the knowledge of stroke. 17 The role of stroke units in improving stroke outcome is also greatly improved if CT scan facilities are available. The use of clinical methods can reduce the rate of stroke misdiagnosis in settings where radiological facilities are not available. They are also invaluable in identifying stroke risk factors thereby improving secondary stroke prevention. There is a need however to make CT scans more widely available to optimise the overall management of stroke. References
|

{kind=link}