 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 4, 2004, pp. 181-184 PATTERN AND MANAGEMENT OF CHEST INJURIES IN MAIDUGURI, NIGERIA N. Ali and B. M. Gali Department of
Surgery, University of Maiduguri Teaching Hospital, Maiduguri, Nigeria Code Number: am04047 Abstract Background: Chest injuries constitute a continuing
challenge to the trauma or general surgeon practicing in a developing country.
This study reviews the pattern and management of these injuries mainly by
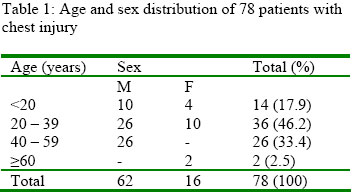
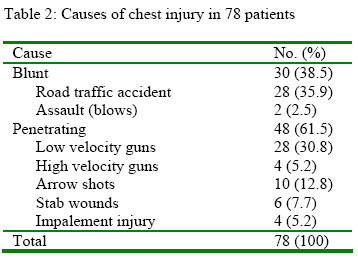
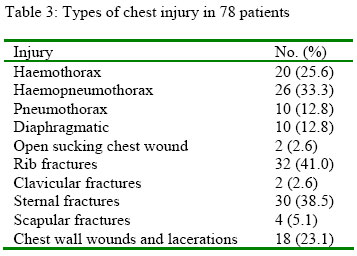
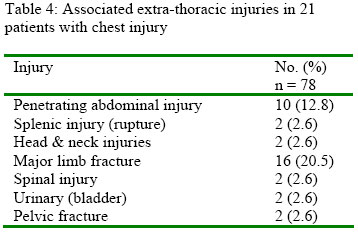
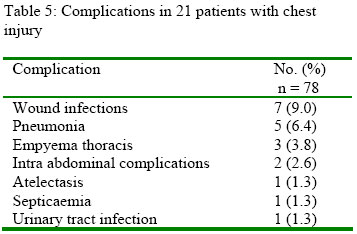
general surgeons. Key words: Chest injuries, pattern, management Introduction Chest injuries are common in the developing countries as elsewhere. The types of injury encountered being basically the same as in other parts of the world, varying only in the pattern. These differences are brought about by variations in infrastructure, civil violence, wars and crime. Road traffic accidents (RTA) are the commonest cause of chest injuries in civilian practice accounting for up to 70% in some series. 1, 2 With increasing use of firearms the incidence of penetrating chest injuries are increasing in civil society. 3 They are often associated with other injuries particularly to the abdomen and long bones. 3, 4 This study reviews the experience of a surgical unit, outlining the pattern of injuries and results of management. Patients and Method A retrospective review of 78 patients admitted into the surgical department of the UMTH between January 1997 and December 1999, with chest injuries was under taken. The hospital records were analyzed for age, sex, types and mechanism of injury, associated injuries, management complications and mortality. The diagnosis was by clinical history, physical examination and abnormal chest radiographs at the accident and emergency unit. Chest injuries were considered as both blunt and penetrating affecting the chest wall, pleura, lungs, lower respiratory tract or contents of the chest e.g. oesophagus, heart and great vessels. Those with minor superficial cuts on the chest wall or bruises were excluded. Results There were 62 males and 16 females, giving a male to female ratio of 3.8:1. The age range was 5 – 67 years (Table 1) with a mean of 32.28 years. Most the injuries were penetrating 48(61.53%), of these; 24(30.76%) were due to low velocity guns, 10(12.8%) had arrow shots and 6(10.34%) were stabbed wounds. There were four cases each (5.13%) of impalements and high velocity gunshot injuries (Table 2). Thirty patients (38.46%) sustained blunt injuries as result of RTA and their commonest problems were rib fractures and pulmonary contusions. All the patients had chest radiographs done; the commonest abnormal findings were rib fractures (32), haemopneumothorax (26), haemothorax (20), pneumothorax (20) and chest wall wounds in 18 patients (Table 3). There were 4 patients with penetrating cardiac injuries from arrow shots. The commonest extra-thoracic associated injuries were limb fractures 32 and penetrating abdominal injuries in 20 (Table 4). Majority of the patients 44(56.4%) required only tube thoracostomy as definitive treatment and 24 (30.77%) and 14(17.95%) required a combination of wound excision, debridement, analgesics, antibiotics and tetanus prophylaxis. These groups were closely observed for any deterioration. Six (7.7%) patients had exploratory laparotomy and splenectomy was done for two who had blunt thoraco-abdominal trauma. Four (5.2%) patients had thoracotomy by the posterolateral approach through the 5th left intercostal space. Two had primary repairs of the bladder on account of multiple arrow shots. The other two had multiple perforations of the ileum and mesentery. They had resection of devitalized bowel and primary anastomoses along standard lines. Ten had diaphragmatic rupture, repaired through the abdomen. Complications developed on 21 occasions (Table 5). Wound infection in 7, pneumonia in 5 and empyema thoraces in 3. Other less frequent but significant complications included two patients with septicaemia, one with atelectasis and two with urinary tract infection (UTI). They were treated successfully with antibiotics and chest physiotherapy, which was employed for all patients, before and after removal of chest tubes. Out of six patients with associated abdominal trauma, 2 developed prolonged ileus, which resolved with nasogastric suction and intravenous fluids. Isolated chest injuries were found in 36 patients (46.15%) with rib fractures found in all of them. The mean period of closed thoracostomy tube drainage was 10 days. The mean duration of hospital stay was 21 days, excluding those with long bones and pelvic fractures. Both periods were longer in the multiple injured and those with penetrating chest injuries. Two patients died following emergency thoracotomy. The mortality rate was 2.56%. Discussion Chest injuries are common reasons for emergency medical care. In civilian practice, chest trauma is commonly caused by road traffic accidents. Most of the injuries are found among young adult males between the ages of 20 and 40 years the very productive period of life. 3-5 The majority of these injuries are blunt except in areas where there is easy access to high velocity or low velocity guns, knives and arrows. With increasing urbanization and its attendant high crimes rate, penetrating chest injuries are becoming more common in civilian practice. 3, 6 Of the 78 patients in this study, 48 had penetrating and 30 had blunt chest injury. The pattern of causes, mechanism and nature of injuries are similar to other studies.7 These uncontrolled surgical events cause injuries ranging from simple rib fractures to sucking chest wounds, pericardial tamponade, haemopneumothorax and other life threatening injuries. The derangement in respiratory movement, hypoventilation, hypoxia, respiratory acidosis, shock and consequent cardiac dysfunction will depend upon the offending weapon and amount of energy transferred. The worst out come is usually associated with high velocity gunshot and blast injuries. 8 Morbidity and mortality increase when another system is involved. Cooper and Miltello reported a mortality of 30 – 35% when two or more systems are involved. 4 The high incidence of penetrating chest wounds in this study is explained by the high rate of crime in northern Nigeria recently and conflict between farmers and cattle rearers. Most of the wounds were caused by locally made low velocity guns and arrows. Those who had blunt injuries were mostly involved in road traffic accidents another common feature of bad roads in this environment. Simple or multiple rib fractures with flail segments were common, blunt abdominal and long bone fractures were the commonest extrathoracic associated injuries in keeping with the general trend. 2-4 The majority of our patients 74 (97.44%) did not require thoracotomy as definitive treatment. The site of intrapleural drain was the 6th intercostal space mid axillary line, unless where there was a specific contraindication e.g. a contaminated wound and the 2nd intercostals space mid clavicular line, when only pneumothorax was present. Tube thoracostomies were inserted along standard lines but improvised, using size 22F Foleys catheter as chest tubes. Additional holes were created at intervals on the catheter and directed upwards into the pleural cavity to drain both air and blood. A Redivac bottle was used in place of a standard bottle and underwater seal drainage established with the tubing of an aldone bag. All the junctions between the tubes were made airtight using adhesive plaster. These improvised tubes worked perfectly in all our patients with only minimal insignificant pneumothorax and no mortality. The average duration of drainage was 10 days. There were 4 thoracotomies during the study period, 2 for an arrow shot in the heart chamber and the third and fourth following massive haemothorax. The latter two died of exsanguination. In war wounds Zachariah established that thoracotomies are very common accounting for up to 71% of cases and tube thoracostomies for 29%. 8 The apparent low incidence of tube thoracostomy as definitive treatment in this study as compared to others is the inclusion of those major chest wall laceration (n = 18), where the contents of the chest were minimally or not affected. Thoracic surgeons generally agree that most patients with especially penetrating chest injuries could be managed adequately by closed thoracostomy tube drainage alone. 2, 3, 6 Inci et al reported the percentage to be between 62.1 and 91.4. 3 Close monitoring of the bluntly injured patient is paramount with repeated examination, radiographs, aortography, electrocardiogram, and computed tomography of the chest and blood gas analysis as appropriate to detect changes. 9 The importance of life support systems cannot be overemphasized. Our patients received basic care with intensive care support. Most of the patients were not severely injured except when there was a major associated extrathoracic injury. They responded favourably to measures that were well within the competence of general surgeons in a hospital remote from those staffed by thoracic surgeons and facilities. The mortality was 2.56% similar to other studies.10, 11 The small number of patients in this study is a reflection of poor access to health facilities in this area. With improvement in communication and emergency services, better results on more severely injured patients can be expected. Reference
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}