 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 4, 2004, pp. 185-187 PATTERN OF CORNEAL OPACITY IN IBADAN, NIGERIA A. O. Ashaye and T. S. Oluleye Department of Ophthalmology, UniversityCollegeHospital, Ibadan, Nigeria Code Number: am04048 Abstract Background: The prevalence and causes of corneal
blindness vary from one region of the world to another. There is even
variation within the developing countries of Africa.
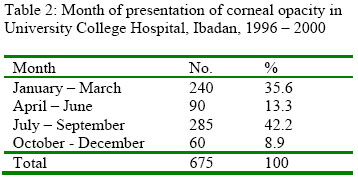
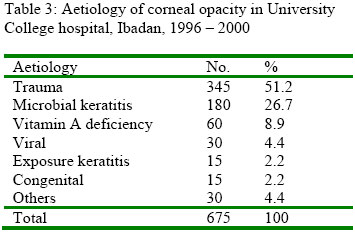
Key words: Cornea, opacity, blindness Introduction The cornea is exposed to the atmosphere and so often suffers injury, inflammation or infection. Corneal opacity results from a process, which upset its anatomy and physiology. Because the cornea is such a specialized structure, any inflammation or injury is likely to cause some permanent damage or scar. The scar tissue is white and opaque, while healthy corneal tissue is transparent. Corneal disease is common in the tropics1 and in developing countries. Indeed the prevalence of corneal scar in any community is a good indication of the general health, hygiene and nutrition of that community. 1 Corneal scar is a leading cause of blindness in Africa after cataract and glaucoma. 2 Corneal scar from measles, vitamin A deficiency, the use of harmful traditional eye medications and ophthalmia neonatorum are the major causes of blindness in children in low-income countries. 3 Ocular trauma and corneal ulceration are significant causes of corneal blindness that are often underreported, but may be responsible for 1.5 – 2.0 million new cases of monocular blindness yearly. 4 The prevalence and causes of corneal blindness vary from one region of the world to another. There is also variation within the developing countries of Africa. Environment and availability of ophthalmic services and general health care are factors that contribute to this variation. 5 No community-based studies have been done to determine the prevalence and causes of corneal opacity in the south western part of Nigeria. As a preliminary to community based study to identify the relative importance of known causes of corneal blindness as seen in the south western part of Nigeria, the aetiology of cases seen in hospital was determined. Patients and Methods A retrospective review of cases with diagnosis of corneal opacity attending the eye clinic of the UniversityCollegeHospital, Ibadan, Nigeria between 1996 and 2000 was carried out. Such cases would have been referred from various clinics within and outside this teaching hospital such as paediatric outpatient and children emergency room. Information sought included, age at presentation, sex, time of presentation visual acuity, and aetiology of corneal scar. Statistical analyses were done, using proportions and percentages to summarize the data. Results There were 3,573 new patients seen in the eye clinic of University College Hospital Ibadan (UCH) during this period of which 675 subjects (18.9%) had corneal opacity. The peak age of presentation was 0 – 10 years (46.7%) (Table 1). The periods of January to March, and July to September were noted to be the peak periods of presentation (Table 2). Trauma (51.1%), microbial keratitis (26.7%) and vitamin A deficiency (8.9%) were the main causes of corneal opacity. Other causes found were viral keratitis, exposure keratitis, and other less frequent causes like opacity following surgery, pterygium and vernal conjunctivitis (Table 3). Almost half (48.9%) of the eyes with corneal opacity seen in this study were blind that is, had visual acuity less than 3/60 after treatment. Discussion Corneal disease is the third most common cause of blindness in tropical countries after cataract. 2 Children and young adults are mainly affected as shown in this study. In a study of an urban population in India, a similar result was found. 6 The finding of a male preponderance with a ratio of 3:1 is similar to what was found in Togo, 7 a neighbouring country. There were two peak periods of presentation in the study, January to March and July to September. The first peak coincides with the dry season, with its accompanying dry, dusty environment, and the likely increase in the incidence of measles while the second peak coincides with the harvesting season when farmers are likely to get injured on the farm. The dry season presentations suggest an increase in incidence of corneal disease from vitamin A deficiency disease. No case of bilateral blindness was found in the study. Corneal blindness is often underreported but may be responsible for 1.5 - 2.0million new cases of monocular blindness every year. 4 In Kenya, Tanzania9 and Sudan10 corneal opacity from trachoma was a major cause of low vision and blindness. In the present study trauma is a major cause of corneal opacity. There is a suggestion that trauma and microbial keratitis are important causes of corneal opacity in patients seen in this hospital, which serve a predominant agricultural population. It was found in Nepal8 that the most common cause of corneal ulceration was trauma. Gara and Rao in India found that corneal infections are responsible for a large proportion of corneal scar and that corneal scar was the most common indication (28.1%) for corneal transplantation, of which keratitis accounted for 50.5%. 11 In Botswana, corneal opacity was reported to be the second most common cause of unilateral and third leading cause of bilateral blindness. 12 In Nigeria, Nwosu found that trauma predispose to uniocular blindness13 and visual impairment, while in the Gambia, 14 non-trachomatous corneal opacity and phthysis bulbi cause about 20% of blindness. WHO, 15 Waddell16 and O’Sullivan et al, 17 reported that in children, xerophthamia, ophthalmia neonatorum and less frequently herpes simplex infection and viral kerato conjunctivitis are responsible for corneal blindness. The use of traditional eye medicines is a major risk factor in the current epidemic of corneal ulceration in developing countries. 18 Because of the difficulty of treating corneal blindness once it has occurred, public health prevention programmes are the most cost-effective means of decreasing the global burden of corneal blindness3. There is a need for communities based study on the aetiology of corneal opacity and plan a programme for prevention of the major causes. References
Copyright 2004 - Annals of African Medicine |

{kind=link}
{kind=link}
{kind=link}