 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 3, No. 4, 2004, pp. 188-191 DERMATOLOGICAL MALIGNANCIES IN KANO, NORTHERN NIGERIA: A HISTOPATHOLOGICAL REVIEW O.Ochicha, *S.T. Edino, A.Z. Mohammed and A.B. Umar Departments of Pathology and
*Surgery, BayeroUniversity and Aminu Kano Teaching Hospital, Kano, Nigeria
Code Number: am04049 Abstract Background: Globally,
dermatological malignancies are among the most common form of cancer but there
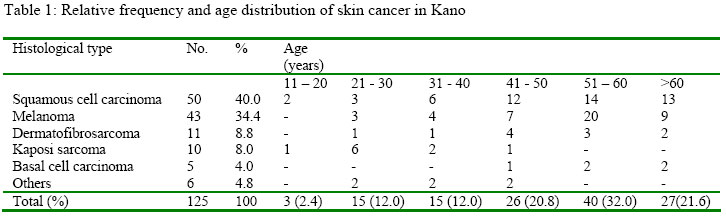
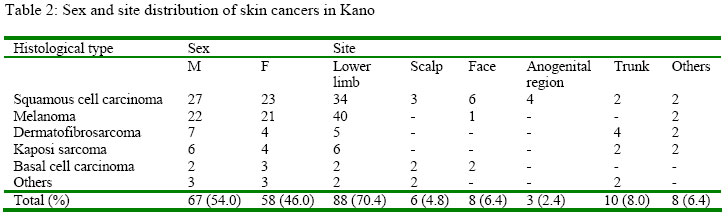
has been no formal study in our locality. Key words: Skin cancer, squamous cell carcinoma, melanoma Introduction Malignant skin tumours are among the most common form of cancer, 1, 2 in fact in White populations it is the commonest malignancy and the incidence is rising. 3, 4 In the last four decades the prevalence of Melanoma in White Americans has increased by over 300%. 4, 5 Among the darker pigmented peoples of the developing world the incidence is much lower. 1, 2, 4 The major reason for this racial difference in the distribution of skin cancer is the protection from ultra violet radiation provided by melanin in the darker pigmented races. 1 - 3, 6 This racial disparity of skin cancer is not only evident in prevalence but also histological types2, 7-12. While Basal cell carcinoma is undisputedly the commonest dermatological malignancy among Caucasians in Europe, North America and Australia, 7, 8 In Africa several studies reveal a preponderance of squamous cell carcinoma. 1, 2, 9-12 Even among Africans there are significant differences in the pattern of skin cancer. Plantar melanomas are quite common in sub-Saharan Africa but much less common among African-Americans. 4, 5 In Tanzania Kaposi sarcoma is the second commonest dermatological malignancy whereas melanomas are more common in Nigeria. 9, 11-13 Similarly there are notable regional differences in the prevalence of skin malignancies within Nigeria. 11-13 In Jos skin tumours comprised only 6.81% of all cancers while in Maiduguri they accounted for up to 20.9%. 11, 13 Thus it is obvious that skin cancer data from other parts of the country may not reflect the pattern in Kano. Hence it is pertinent to document and evaluate the pattern of malignant cutaneous tumours in Kano, the largest Northern Nigerian city. Materials and Methods This is a retrospective study of all histologically diagnosed malignant skin lesions seen over a five year period (1998-2002) at the histopathology laboratories of Aminu Kano Teaching Hospital, MurtalaMohammedSpecialistHospital and NationalOrthopaedicHospital, Kano, Nigeria. These hospitals are the only tertiary health institutions offering histopathology services to Kano and the neighbouring Jigawa states. Histology slides of cases within the study period were reviewed and clinical data (age, sex, and site) obtained from the histopathology request forms/register. All slides had been routinely stainedwith haematoxylin/eosin and special stains like Masson-Fontana employed where necessary. In addition, histopathology records of all malignancies during the study period were reviewed to determine the relative frequency of skin cancer. Results One hundred and twenty five histologically diagnosed dermatological malignancies were reported during the period under review. This comprised 12.7% of all histologically diagnosed cancers in Kano. Sixty seven (54%) were males and 57 females (M: F=1.2:1) Table 1 shows the relative frequency and age distribution of the various skin malignancies in Kano. Squamous cell carcinoma was the most common constituting 40% followed by melanoma 34.4% and dermatofibrosarcoma 8.8%. Malignant skin tumours most frequently occurred in the 6th and 7th decades and there were no cases in the first decade of life. Table 2 shows the site distribution of skin malignancies. The lower limbs were by far the commonest site accounting for over 70%. More than two thirds of our squamous cell carcinomas (34 cases - 68%) were well differentiated tumours secondary to chronic leg ulcers. Over 90% (40 cases) of our melanomas were nodular hyperpigmented plantar tumours and all were >10mm in thickness. Half (5) of the Kaposi sarcomas cases in this series were from human immunodeficiency virus (HIV) positive patients. Discussion Dermatological cancers comprised 12.7% of all malignancies in Kano. This is comparable to 12.3% in Zaria, 14 a neighbouring city but higher than 6.81% in Jos11 and lower than 20% in Maiduguri. 13 Even with the differing figures from these Nigerian studies, the relative frequency of skin cancer is much lower than in White populations where skin cancer accounts for over half (>50%) of all malignancies especially among those living in sunny tropical/subtropical climates and the incidence continues to rise alarmingly. 1,3,6,15 Lower levels of oncoprotective cutaneous melanin in Caucasians render them more vulnerable to carcinogenic solar ultra violet (UV) radiation particularly from recreational sun exposure, more so with the current depletion of the ozone layer which filters solar UV radiation. 1,3,6,7 While sun exposure is the major aetiological factor in Whites, chronic ulcers and inflammation appear to be leading risk factor in Blacks. 9-11 Numerous reports from Nigeria and other parts of Africa document squamous cell carcinoma (SCC) secondary to chronic ulcers as the commonest cutaneous malignancy. 9-11 This is consistent with our findings in this review where squamous cell carcinoma was the most common accounting for 40%. SCC is also the commonest dermatological malignancy among Black Americans and interestingly in African Albinos. 13,16,17 It is expected that since sun exposure is the major aetiological factor in the hypopigmented African Albinos, 1,16,17 the prevalent histological type among them would be as in white folks, basal cell carcinomas (BCC). 2, 7, 8 Perhaps other non-pigment related genetic factors in Africans render us prone to SCC. BCC comprised only 4% of skin cancers in this review in marked contrast to 70-80% in Whites. 1, 2, 4 Again our findings are comparable to 3.9% in Jos11, 2% in Zaria9 and 2% in Maiduguri. 13 Only two (40%) of our five BCCs occurred in the face in contradistinction to Whites among whom the facial BCC constitutes up to 90%.8 Melanomas are the most lethal cutaneous malignancy accounting for more than three quarters (79%) of all skin cancer deaths. 2 These highly aggressive tumours were the second most prevalent dermatological malignancy in this study constituting 34% which is comparable to other Nigerian studies9,11-13 but relatively more than 5-10% in Caucasians. 1,2 It is noteworthy that although Melanomas comprise a relatively large fraction of malignant cutaneous tumours in Negroids, they are in fact 10-20 times more common among the fair skinned Caucasians. 2,4,5 As in other black populations in Africa and in Diaspora, the sole of the foot was overwhelmingly the commonest site in this study constituting 93%. This plantar predilection of Negroid melanomas has prompted speculation of trauma as an aetiological factor5, 19 whereas among Whites UV radiation again appears to be the major culprit as the sun exposed parts of the body; head, trunk and legs are the favoured sites. 1,2,4,5 Plantar melanomas are less common in black Americans than in black Africans4, 5 presumably because the latter that have lower standard of living are less likely to wear protective footwear. The major prognostic determinant of these deadly neoplasms is the depth of invasion. Melanomas >3.65mm thick have poor prognosis as 60% will develop metastases and die from the disease.4 Unfortunately due to late presentation all our cases were nodular melanomas more than 1.0cm thick in contrast to Melanomas in White people which are predominantly non-invasive - superficial spreading or lentigo maligna. 4, 5 Thus although melanomas are commoner in Whites the prognosis is poorer in Blacks18. A comparative study in South Africa found 20% five year survival for blacks and 42% for Whites. 18 Kaposi Sarcoma (KS) was the 4th most prevalent skin malignancy in our locality comprising 8% of skin cancer which is lower than 11% in Jos11 and 16% in Maiduguri. 13 According to the 1999 national HIV sentinel survey, the north central and the north east geographic zones to which Jos and Maiduguri respectively belong have higher HIV infection rates (7.0% and 4.5%) than Kano (3.2%). 20 This may explain our relatively lower rate of Kaposi sarcoma as only half of our cases were HIV positive. In Tanzania where HIV infection rate is even higher, Kaposi sarcoma was the second most common dermatological cancer after squamous cell carcinoma.10 Similarly in Zimbabwe, there has been a significant rise in skin cancer due to increased number of HIV related Kaposi sarcoma. 21 Thus it is obvious that successful HIV control will go a long way to reduce the incidence of this vascular malignancy. References
The following images related to this document are available:Photo images[am04049t1.jpg] [am04049t2.jpg] |
| |||||||||

{kind=link}
{kind=link}