 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
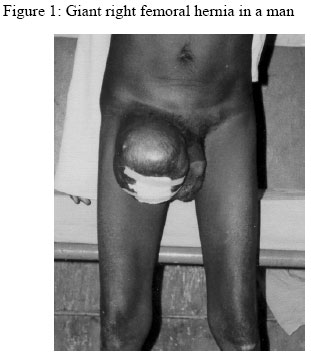
Annals of African Medicine, Vol. 3, No. 4, 2004, pp. 197-198 GIANT FEMORAL HERNIA IN A MALE M. M. Dauda and *N. M. Said Departments of
Surgery, AhmaduBelloUniversity Teaching Hospital, Zaria
and *Federal Medical Centre, Gusau, Nigeria Code Number: am04052 Introduction Giant (voluminous) femoral hernia is defined as hernia that exceeds the size of a fist.1 Eighty percent of giant groin hernias are usually indirect inguinal hernias. Femoral hernias are rare in Africans.2 The reported incidence in Canada is approximately1.5%of all hernias. Femoral hernia presents with the greatest risk of incarceration and strangulation.3 A 52-year old man presented with a 5-years history of a progressive right inguinal swelling. The swelling reduces spontaneously on lying flat, until a year earlier when it became irreducible. He had no cough, no urinary symptoms and had normal bowel habits. There was no abdominal distension. Physical examination showed temperature of 36.20C and no pallor. The abdomen was scaphoid. There was a large right groin swelling below and lateral to the pubic tubercle displacing the penis and the scrotum to the left. There was visible cough impulse. The swelling was non-tender and could only be partially reduced (figure 1).Regional lymph nodes were not enlarged. Rectal examination was normal. Examination of other systems was normal. Chest X-ray, urinalysis, stool microscopy and serum electrolytes and urea were normal. At surgery general anaesthesia, and through a vertical incision across the inguinal ligament ( extended over the swelling), the findings were a large femoral defect of 4cm, and a huge sac containing 80cm of small intestine. There were tortuous and distended right femoral vein, and the lacuna and pectineal ligaments were weak. The small intestine was carefully separated from and reduced without difficulties. The sac was excised and the defect repaired. Post operative recovery was uneventful and the patient was discharged 14 days later. He has remained well at 28 months of follow up. Discussion Despite the rarity of femoral hernia in men, giant femoral hernias occur more frequently in men than women.1 Reports from parts of Nigeria3 indicate that these hernias present with the greatest risk of incarceration. However, despite there greater risk of incarceration, reports from Ghana4 indicates a low incidence of strangulation. Our patient had the hernia for 5 years and was incarcerated for over a year without strangulation. Giant femoral hernias present special surgical problems, largely because of the advanced age of the patients, poor general condition, obesity, repair of large defects and difficult peri- operative management.1 Despite the large volume of the hernia in this report, the relatively young age, good stature and general good health, resulted in successful recovery. Recurrence following primary femoral hernia repair occur in 6.1%, with 55% occurring within a year.5 There has been no recurrence in this report after over 2 years of follow up. Acknowledgement We are grateful to Dr. E.A. Ameh, Consultant Paediatric Surgeon, for offering useful suggestions and criticisms. References
Copyright 2004 - Annals of African Medicine |

{kind=link}