 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
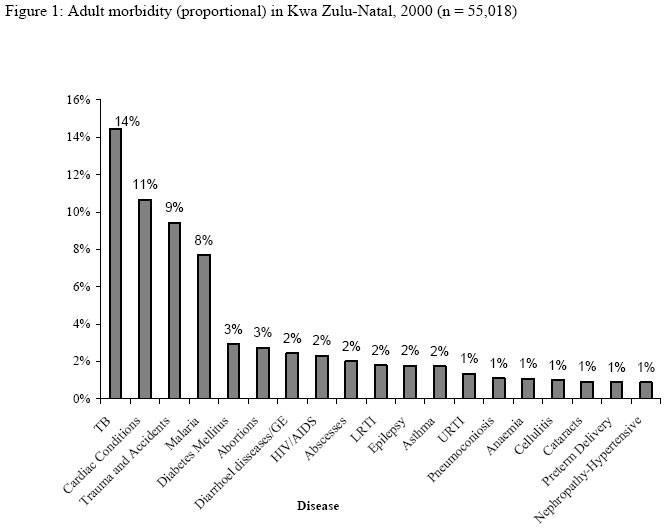
Annals of African Medicine, Vol. 3, No. 4, 2004, pp. 199-200 DISEASE BURDEN ON KWA ZULU-NATAL HOSPITALS- 2000 Monjurul Hoque Medical Manager, Empangeni Hospital, Private Bag X20005, Empangeni 3880, South
Africa Code Number: am04053 Dear Editor Morbidity and Mortality data are the basis for assessing the health status of population and are necessary for public health services and policies. The aim of health services is to improve the health status of the population through reduction of morbidity and mortality. The burden of diseases in the community and health facility directs appropriate planning for services, resources allocation etc. Based on the “Ten points plan” developed by the National Department of Health in the strategic framework (1999-2004), reduction of morbidity and mortality rates through strategic intervention ranks top on the list.1 The true measure (epidemiological purpose) of disease profile of a population would be to conduct a Community based survey or measure. Facility based measures (user’s selection) thus fulfil some management objectives. Facility-based data collection was conducted in Kwa Zulu-Natal (KZN) during 2000 (January to December).A data collection tool was developed along with a guideline to collect Hospital in-patient data (discharge diagnosis of all patients). Thereafter requested to all hospitals of the Province to collect daily, summarize monthly and then submit to Epidemiology unit. The data was divided into two groups – Adults (>13 years) and children. Adult discharges data (morbidity) are presented here. A total of 32 hospitals (Tertiary, Regional and District) among 60 public hospitals in KZN contributed towards compilation of the Provincial hospitals disease burden. A total of 55018 discharge data from the participating hospitals were analyzed and presented. Incomplete submissions were excluded. This data does not represent the province due to poor response rate. Re-admissions during the data collection period, referrals to other facilities, multiple diagnoses might have influenced over estimation of condition/s. Private and other facilities were not included in the study. Thus this is considered as crude estimation of burden of diseases on health facilities. Tuberculosis (TB) is the commonest cause (as a single diagnosis) of hospitalization (14%) among the reported conditions followed by Cardiac Conditions (11%), Trauma and accidents (9%), Malaria (8%), Diabetes (3%) and Abortions of all types (3%) respectively (Figure 1). In the year 2000 the crude disease burden of KZN clearly demonstrates the predominance of communicable conditions. While non-communicable diseases accounted for approximately 30% of morbidity in KZN (after grouping the single causes). It is thus the evidence of double burden of diseases. KZN within the context of South African Society, like many other developing societies is pre-eminently a society in epidemiological transition and this is reflected in its diseases burden. Reasons for high incidence of TB in KZN could be contributed tp high incidence of HIV infection, emergence of multi-drug resistance TB (MDR), inadequate or poorly implemented control program resulting in poor management of cases, poor socio-economic circumstances, improved surveillance system and access to care. This finding is higher than the 1995 Hlabisa Hospital TB admission2 (8.3%) in KZN. It is also estimated that SA has a TB/HIV co-infection rate of 254/100,000.3 Trauma is the third most common (9%) cause of hospital burden in KZN. In 1992, 14.4% of all KEH VIII admission was due to Trauma. 4 HIV related conditions might have been underestimated due to limitation of reporting. Higher proportion of hospital admissions for abortions may be due to failure of termination of pregnancy and adoption of other means. In order to estimate the disease profile and monitor health sector achievements of its goals, a representative sample survey or sentinel surveillance sites should be developed with comprehensive demographic and epidemiological data items so that risk groups, risk areas, morbidity and mortality trends are identified for implementation of appropriate interventions. References
Copyright 2004 - Annals of African Medicine
|

{kind=link}