 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
RADIOGRAPHIC FEATURES OF PULMONARY TUBERCULOSIS AMONG HIV PATIENTS IN MAIDUGURI, NIGERIA 1A. Ahidjo,2H Yusuph, 1A. Tahir Departments of 1Radiology and 2Medicine, University of Maiduguri Teaching Hospital, Maiduguri, Nigeria Reprint requests to: Dr Ahmed Ahidjo, Department of Radiology, University of Maiduguri Teaching Hospital P. M. B. 1414, Maiduguri, Borno State, Nigeria. E-mail: ahmedahidjo@hotmail.com Code Number: am05003 Abstract Background: Tuberculosis infection may develop at any stage
of HIV infection. Pulmonary tuberculosis produces a broad spectrum of radiographic
abnormalities among HIV patients. Key words: HIV, pulmonary tuberculosis, radiographic features, Nigerians Résumé Fond: L'infection de tuberculose peut se développer à n'importe
quelle étape de l'infection par le HIV. La tuberculose pulmonaire produit un
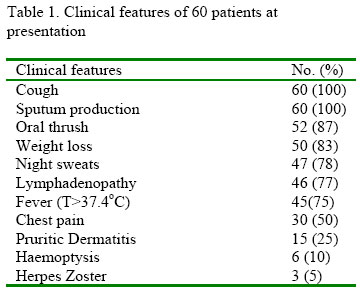
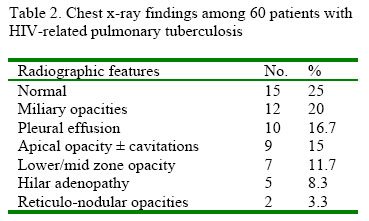
large éventail des anomalies radiographiques parmi des patients d'VIH. Introduction The recent increase in the prevalence of tuberculosis (TB) globally, particularly in Africa has been attributed to the increase in number of human immunodeficiency virus (HIV)-infected patients.1, 2 There is rising incidence of TB, especially pulmonary TB (PTB) in HIV-infected patients as well as a high rate of HIV in patients suffering from tuberculosis in Nigeria and other parts of the world.3 The reported HIV-seroprevalence rates among TB patients in Nigeria range between 5.3%and 36%, 4-7 whereas the reported HIV-seroprevalence rates range between 12% and 55% in Africa and 39% worldwide.8 The clinical manifestations of PTB are productive cough, oral thrush, weight loss, night sweats, fever, chest pain and herpes zoster. Tuberculosis infection may develop at any stage of HIV infection.3 Pulmonary tuberculosis produces a broad spectrum of radiographic abnormalities among HIV patients. These include consolidation of the middle or lower lobe or anterior segment of the upper lobe, cavitation, pleural effusion, hilar and mediastinal adenopathy, miliary disease and a normal chest radiograph in the primary phase of the disease .4, 5,9 Typical lesions are seen in post-primary TB, these include upper lobe fibrosis, consolidation and cavitation. ,9,10 The aim of the study was to document the radiographic features of pulmonary tuberculosis among HIV-positive patients in Maiduguri, northeastern Nigeria. Materials and MethodsThis was a cross-sectional study carried out at the University of Maiduguri Teaching Hospital, Maiduguri, Nigeria from September 2001 to August 2002. A total of 60 consecutive patients with sputum smear positive pulmonary tuberculosis, positive for HIV antibodies as detected by enzyme-linked immunosorbent assay (ELISA) (Genscreen HIV1/HIV2 version 2. Sanofi-Pasteur) and confirmed by immonocomb II (IMMUNOCOMBFIRM) (HIV1/HIV2 combfirm Orgenics) were studied. Patients on immunosuppressive therapy, antiretroviral therapy longer than one week, antituberculous therapy for more than one month and those who denied consent as well as patients with diabetes mellitus, chronic renal failure, nephrotic syndrome, sickle cell disease and widespread malignancies were excluded from the study. Standard posteroanterior chest radiographs were obtained with film-screen at 90–140 KVp in all patients. All films were reviewedindependently bytwo consultant Radiologist. The data obtained were analyzed using SPSS version 11.0. ResultsThirty four males (56.7%) and 26 females (43.3%) were enrolled into the study. The age range was 18 - 55 years with a mean (± SD) of 33.9 ± 8.42 years and median of 33 years. The major clinical features at presentation are shown in table 1. The duration of symptoms prior to presentation ranged from 3 weeks to 8 months. Using the 1993 CDC Surveillance Case Definition of AIDS, 16 26 of the patients were in category C3, 32 in C2 and only 2 in C1. The distribution of radiographic features of PTB is shown in table 2. Normal radiographs constitute the highest number of patients (25%), followed by milliary opacities in 20%. Reticulonodular opacities (3.3%) and hilar adenopathy (8.3%) were the least radiograghic features seen. Discussion The mean (± SD) age of the patients in this study is similar to the observations of other workers 11 - 13 and Hsieh et al14 in Taiwan who reported a similar age distribution among HIV–associated PTB patients. This corroborates the fact that HIV is more common in people in their productive and sexually active age groups.15 The male: female ratio of 1.3: 1 shows the near unity in sex distribution of HIV infection in Nigeria. However, it differs from the findings of other workers in other parts of the world16 and Nigeria11 - 13 who reported male preponderance. This may be due partly to time difference between this and other studies. However, polygamy in this part of Nigeria, early female marriages, freedom to remarry after divorce or death of a spouse might have contributed to this disparity. The chest X-ray findings in this study are similar to those of Awoyemi et al17 in Ibadan. However, the higher rates of normal radiographs in our patients may be related to immune status, as immunosuppressed patients may not mount adequate immune response to M. tuberculosis. The finding of normal chest radiograph in our HIV-related PTB patients is similar to others. 4, 16, 18, 19 Kawooya et al9 reported a prevalence of 98.7%, 43.3%, 41.3%, 25.3% and 2% for lung opacities, cavitation, lymphadenopathy, pleural effusion and miliary pattern, respectively among HIV-seropositive patients studied in Uganda. These high rates may be accounted for by other conditions like diabetes mellitus, malnutrition and other infections as well as environmental socio-economic factors which also cause immunosuppression – a factor they have in common with HIV. Similarly, Woodring et al 20 in their series found a prevalence of 37.5%, 25%, 3.1%, 6.2% and 17.2% for consolidation, cavitation, military, adenopathy and pleural effusion, respectively. This study included only patients that were non-immunocompromised which may explain the low rates of military pattern. Majority of patients in our study had normal chest radiographs. Absence of changes in chest radiographs should not exclude the diagnosis of PTB. References
The following images related to this document are available:Photo images[am05003t2.jpg] [am05003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}