 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
DAY-CARE PLASTIC SURGERY IN NIGERIA: COPING WITH LIMITED RESOURCES J. N. Legbo and W. Ek. Opara Department of Surgery, UsmanuDanfodiyoUniversity Teaching Hospital, Sotoko, Nigeria Reprint requests to: Dr J. N. Legbo, Plastic and Reconstructive Surgery Unit, Department of Surgery, Usmanu Danfodiyo University Teaching Hospital, P. M. B. 2370, Sokoto 840001, Nigeria. E-Mail: legboj@yahoo.co.uk Code Number: am05005Abstract Background: The main problems facing acute surgical services
in most countries are shortages of resources and finance, and long waiting
lists. The concept of day–care surgery has been well established since the
early nineties. Since then, enthusiasts have also indicated that day–care
surgery represents a safe, cost–effective and efficient practice. Résumé Fond: Les problèmes principaux qui charactérisent les services
chirurgicaux aigus dans la plupart des pays sont des manques de ressources
et de finance, et également de longues listes d’attente. Le concept de chirurgie
d'assistance sociale a été bien établi depuis le début des années quatre-vingt-dix.
Depuis, les fervents ont indiqué aussi que cette chirurgie d'assistance sociale
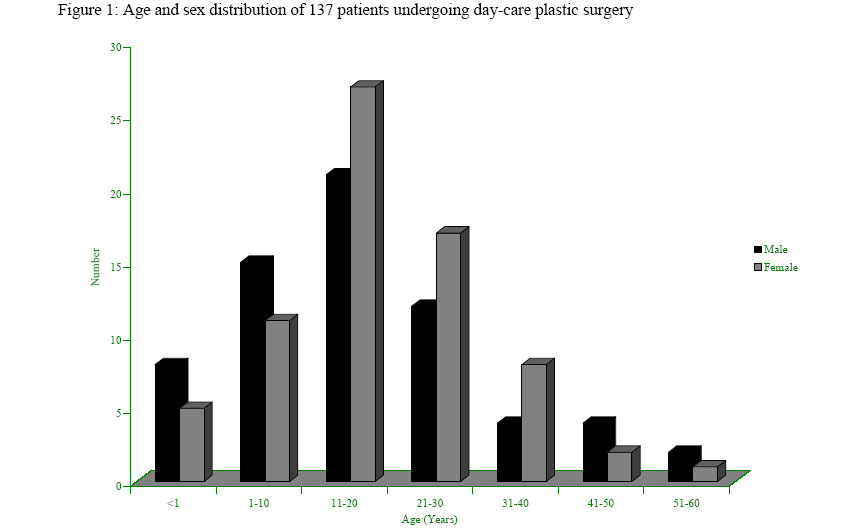
représente une pratique sûre, rentable et efficace. Introduction Improvements in anaesthesia and pain control, advent of minimally invasive surgery and the changing attitudes of recovery after surgery have all promoted the expansion of day-care surgery worldwide.1 In recent years, it has become apparent that many of the common plastic and reconstructive surgical procedures are ideally suited for day-care. 2 The main problems still facing health services in most developing countries are ever-increasing population, poor communication facilities, slow economic growth and poor health financing with its accompanying shortages of both human and material resources. 3, 4 In the area of plastic and reconstructive surgery, the principal problem arises from the care of the dressing for skin grafts and flaps, and the removal of the very tiny sutures. This peculiar challenge creates the need for experienced personnel especially trained in the techniques and it is important that a dressing clinic be mounted as a special support for day-care plastic surgery. 2 It is obvious in most health institutions in Nigeria that the surgical demands of our fast expanding population can hardly be met by the available in-patient facilities. 2, 4 Apart from the reduction of the cost of treatment, day-care surgery reduces surgical waiting list, nosocomial infections as well as the psychological effects of hospital admission. 1-4 Day-care plastic surgery therefore serves as a reasonable option for an increasing number of plastic and reconstructive procedures in a wide range of patients in Nigeria today. Aside from the initial reluctance in accepting this mode of surgical treatment in Nigeria, and the numerous socio-economic set back, it is heartwarming to note the reports of successful outcome in series of procedures done as day cases, including plastic and reconstructive surgery. 3-5 This study evaluates the scope and problems of day-care plastic surgery in a resource-limited tertiary institution in Nigeria. Patients and MethodsThis is a 3-year retrospective study of all day-care plastic surgical patients operated upon from January 2001 to December 2003 at the Usmanu Danfodiyo University Teaching Hospital, Sokoto. The hospital numbers of such patients were sought from the theatre register while the case notes were subsequently retrieved from the medical records department. Information extracted included the patient’s demographic data, diagnosis, surgical procedure, anaesthetic technique, postoperative analgesia, postoperative complications and follow-up. Prior to surgery, all patients were seen at the plastic surgical out patient clinic by the consultant plastic surgeon or an experienced resident. Careful preoperative assessments were made to establish the diagnosis and also to determine patients’ suitability or otherwise for day-care plastic surgery. The exclusion criteria followed standards methods1-3, 6, 7. Relevant investigations were done for all the patients. All patients (or their parents/relations) were properly counseled by doctors on the type of surgery and possible anaesthesia. Appropriate instructions were given for preoperative fasting and the patients told to report to the relevant surgical ward at staggered times from 8.00 am to 12.00 pm on the day of surgery. From their respective wards, patients were subsequently transferred to the theatre for joint reassessment by both the plastic surgical as well as the anaesthetic teams. Operations were done either by the consultant plastic surgeon or an experienced resident. Postoperatively, all patients were observed at the recovery room before transfer to their respective wards. Patients were then discharged (after review in the wards) with adequate instructions, postoperative medications and out patient clinic appointment. Where necessary, dressings were done in the clinics, and sutures were removed between the 3rd and 10th postoperative days. Information on individual patient were entered into a proforma and subsequently transferred into the computer for analysis. Results A total of 148 procedures were done in 137 patients. This represented 37.3% of all procedures (397) and 36.5% of all patients (375) treated in the unit within the same period. The ages ranged between 2 weeks and 58 years (mean = 23.1 years). There were 66 (48.2%) males and 71 (51.8%) females, giving a male: female ratio of 1: 1.1. Over half of the patients (56.2%) were aged between 11 to 30 years. Figure 1 shows the age/sex distribution of all patients. A wide range of surgical procedures was carried out for varying surgical problems. The most frequently performed procedure was lipomectomy (11.7%), followed closely by biopsy of skin lesions (10.9%), incision of tongue tie ( 10.2% ), excision of breast lump ( 9.5% ), reconstruction of nose or ear (8.8%), ganglionectomy (8.0%), keloid excision, facial scar revision, grafting of cutaneous ulcers (5.8% each), and others. Table 1 shows the scope of plastic surgical problems encountered. Majority of the patients were in the American Society of Anaesthesiologists (ASA) category I and resided within Sokoto metropolis or the surrounding towns and villages, but the exact distances of their residential areas to the hospital were not adequately indicated in the case notes. Various forms of anaesthesia were employed. In 92 (67.2%) patients, operation was done using loco-regional block by local infiltration with lignocaine. Intravenous ketamine hydrochloride was used in 41 patients (29.9%) while the remaining 4 (2.9%) had inhalational anaesthetics. The duration of surgery ranged from 10 to 95 minutes (mean = 37.4 minutes). Postoperative analgesia was achieved using oral Non Steroidal Anti Inflammatory Drugs (NSAIDS) like paracetamol and diclofenac in 109 (79.6%) patients. Oral narcotic analgesics like tramadol were used in 28 (20.4%) patients. Postoperative morbidity was minimal as complications were observed in only 13 (9.3%) of the patients. This included wound infection in 11 (8.0%) patients, bleeding and pain each in 7 (5.1%) and haematoma in 4 (2.9%) patients. Five patients (3.6%) were readmitted either from delayed recovery from anaesthesia or from postoperative bleeding. No mortality was recorded in the course of the study of follow-up. Follow-up was impressive and ranged from 3 weeks to 2.5 years (mean = 4.25 months). Table 1: Scope of plastic surgical problems in 137 patients undergoing day-care surgery
Discussion Until recently, day-care surgery has remained poorly developed in Nigeria. 4, 5, 8-11 Although this is a fast evolving concept in the developed world, 1-3 it was visited with reluctance in most developing countries (like Nigeria) due to fear of inadequate road/communication network and lack of community support services for the success of the programme. Fortunately, this has given way to wide acceptance by patients and appreciable embrace by medical staff. In Nigeria today, several centers provide day-care in various surgical subspecialties (including plastic surgery) with encouraging results. 4, 5, 8-12 The organizational set up for day-care surgery may differ from one center to another. 1, 2 The day surgery unit, which represents the ideal, is not available in most centers in the developing countries2. The day case ward is a less desirable alternative but may prove an acceptable way of commencing day surgery. At our center, an even less desirable alternative, the general ward is what we had to cope with over the 3-year study period. Despite the fact that the plastic surgery unit of the institution has just been set up, we have been active in providing a wide range of diagnostic as well as therapeutic procedures on day-care basis. In our study, 37.2% of all plastic surgical procedures were done on day-care basis. This figure exceeds the target projected by the Royal College of Surgeons of England in 1985 6 and the 22.7% reported previously in a plastic surgical unit in Nigeria5; but significantly lower than the observations of other authors in Nigeria4 and North America1, 2 where figures nearing 70% have been quoted. Day-care surgery is not cost saving for the patient alone, but also to the institution. 1-5, 9 Like in most reports in Nigeria4, 10 and elsewhere in the world, 1, 2 most of the procedures were carried out in carefully selected patients of acceptable chronological age group according to known guidelines. 6, 7 In addition, nearly all the procedures were in the minor to moderate category in order to cope with the present level of patient awareness, limited social and medical resources available within the hospital and the communities. This is in consonance with earlier suggestions that procedures be limited to those that cause minimal physiological disturbance, minimal postoperative pain and have little risk of haemorrhage, to enhance safety and retain the confidence of our patients. 2, 4, 6, 7 It is in the same spirit that most of the patients selected were residents of Sokoto and environs. There is a current wave of improved transportation and communication facilities in most communities in Nigeria. Consequently, it is expected that the volume and diversity of permissible plastic and other surgical day-care procedures will increase tremendously to comparable figures with those of the developed countries. In contrast with the experience in a plastic surgery unit in a Nigerian health institution, 5 lipomectomy was the most commonly performed surgical procedure in our study. Most of them were well encapsulated and located mainly at the subcutaneous plane, thereby posing no difficulties in removal. Of interest were 12 (8.8%) patients who presented with partial losses of the nose or ear, resulting mainly from human bite, for which local flap reconstructions were effected. Keloid excision and direct closure or skin grafting was done only in 11 (8.0%) patients in this study. Anaesthetic considerations are of utmost importance in day-care surgery. 13-17 As a policy in many tropical countries, local anaesthetic is preferred in practically all cases for day surgery in adult patients. 2 This is because of its relative safety, rapid recovery and minimal postoperative problems like nausea, vomiting and headache, thereby facilitating faster discharge from hospital. 1-4, 13-17 In addition, local anaesthetic offers some pain relief in the immediate postoperative period. However, with improvements in the modern general anaesthetic agents, recovery following this form of anaesthesia can be both rapid and complete. 4, 15 This promises to increase the frontiers of day-care surgery. In our study, 67.2% of the patients had their procedures done under local anaesthesia. This compares favourably with 74.3%4 and 77.6%5 previously published in Nigeria and elsewhere in the world1, 2. Intravenous ketamine or inhalational anaesthetics were administered mainly to children who usually would not cooperate with local infiltration; or in adults where local infiltration was adjudged unsuitable either by the plastic surgeon or the physician anaesthetist. No patient in this study had spinal or epidural anaesthesia, which are widely used today in Europe for day-care surgery. 13, 18 In the tropics, these forms of anaesthesia are usually employed in rare cases of failed local infiltration, and such patients are usually converted to in-patients2 in order to observe for possible complications such as post-dural puncture headache. Fortunately, the introduction of small gauge conical-tipped needles that result in less dural trauma has significantly reduced the incidence of post-spinal headache. 18 Our mean duration of surgery (37.4 minutes) conforms to the suggested operating time of about one hour. 2, 6, 7 Also of critical importance in day-care surgery is the control of postoperative pain. 19, 20 In our study, this was achieved in nearly 80% of patients using NSAIDS like paracetamol 15mg/Kg body weight in four divided doses, taken for 3 to 5 days. Only about 20% of the patients required oral narcotics, for which tramadol was the most frequently prescribed. Wound infection was the most common postoperative complication observed in our study. This is a departure from the findings of other workers 3-5 where pain was predominant. These observations may not be unrelated to the different surgical procedures embarked upon in the various studies, the influence of socio-cultural factors on the perception and expression of pain, and the fact that most patients have accepted pain as an inevitable consequence of surgery which they are often prepared to accommodate19. Readmission is an indication of failed day-care. Readmission rate was 3.6% in this study and resulted mainly from postoperative bleeding and delayed recovery from anaesthesia. The patient who bled had incisional biopsy for Kaposi’s sarcoma and he did well after crepe bandaging and elevation of the leg. This rate compares well with the 2.4% previously reported in a plastic surgery unit in Nigeria5, and is an indication of good patient selection. In conclusion, this study has demonstrated that day-care plastic surgery in our sub region is feasible, safe and effective. Our findings agree with the findings of others2-5 that detailed preoperative patient assessment and careful patient selection are prerequisites to effective day-care surgery. We are also of the opinion that continual review of practice should focus vision on the ideal, the day surgery unit; or at least the day case ward, instead of the present day-care surgery in the general ward used in most centers in Nigeria. This will allow effective documentation/follow-up and easy assessment of the impact of day-care surgery. Furthermore, the idea of day-care surgery should not be misconceived as a means of conserving resources, but deriving from an intention to develop a high quality service befitting the perceived needs of the public. References
Copyright 2005 - Annals of African Medicine The following images related to this document are available:Photo images[am05005f1.jpg] |
| |||||||||

{kind=link}