 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
BASIC PLASTIC SURGERY SKILLS FOR DISTRICT AND COMMUNITY DOCTORS TO MANAGE BURULI ULCER IN GHANA 1P. Agbenorku, 1M. Agbenorku, 2R. Adator, 3L. Tuuli and 4E. Brobbey1Plastic and Burns Surgery Unit, Department of Surgery, Komfo Anokye Teaching Hospital School of Medical Sciences, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana, 2 E.P.Church of Ghana Medical Centre, Krapa-Ejisu, Ash, Ghana, 3 Presbyterian Hospital, Agogo, Ash, Ghana and 4 Leprosy Control Unit, Ghs-Regional Health Administration, Kumasi, Ghana Reprint requests to: Dr. P. Agbenorku, Plastic and Burns Surgery Unit, Department of Surgery, KomfoAnokyeTeachingHospitalSchool of Medical Sciences, KwameNkrumahUniversity of Science and Technology, Kumasi, Ghana. E-mail: pimagben@yahoo.com Code Number: am05009Abstract Background: The increase in incidence of Buruli ulcer in
Ghana has also been complicated by problems in the care of the patients including
lack of knowledge and training by staff, unwillingness of the staff to handle
the cases
for fear of contracting the disease. Résumé Fond: L'augmentation dans l'incidence d'ulcère de Buruli
au Ghana a été aussi compliquée par les problèmes qui font face au soin des
malades y compris le manque de connaissance et d'entraînement par le personnel,
la mauvaise volonté du personnel pour entreprendre les cas en raison de la
crainte de contracter la maladie. Introduction The increase in the incidence of Buruli ulcer patients in Ghana especially in the Ashanti Region is becoming more of public health and social problem. 1,2 The complicated cases with the increase in their management cost are equally a problem to the plastic surgeon. The results of treatment are better when these patients are seen and managed earlier. More so, the complications and sequel are far less when these patients are treated earlier. 3-8 On the average most of these patients reported to the tertiary health institutions after one year. Some cases reporting early to the district/community health institutions may not be managed properly due to various factors. Some of these factors might be: 10,12
It was therefore thought wise to take up the challenge of training the district/community hospital staff in the management of the Buruli ulcer patients in their own or nearby institutions. The programme was designed and started off on voluntary basis far back in 1996 while sources of funding was being be sought for. 7 In the meantime voluntary teams were organized to various endemic areas in Ghana notably in the Ashanti Region and the Ga District of the Greater Accra Region. In 1998 a voluntary team visited Abor Catholic Hospital and also another one visited Comboni Catholic Hospital at Sogakofe in 1999, both in the Volta Region where there were reported cases of Buruli ulcers. Since 1994 the voluntary teams visited almost regularly institutions such as Agroyesum Catholic Hospital, Nkawie Government Hospital and the Evangelical Presbyterian Church of Ghana Medical Centre, Krapa. The aim of the team was to operate as many as possible Buruli ulcer patients and also to train the local staff to do the same – the Basic Plastic Surgery Skills. However, as much as the team would have wished to continue this good work there was often lack of logistics to continue. In the year 2000 two separate and identical applications were made to 3 organisations, including the American Leprosy Missions (ALM). The later organization replied positively and offered to assist through a Christian based organization. The Evangelical Presbyterian Church of Ghana was selected as the partner organization to help in the conduct of this project. The approved project title was “Basic Plastic Surgery Skills for District/Community Doctors to Manage Buruli Ulcer Patients in Ghana”. With the support of the ALM and the Ministry of Health-Ashanti Region three successful workshops were held:
Purpose of the Workshops The purpose of the Workshops was to:
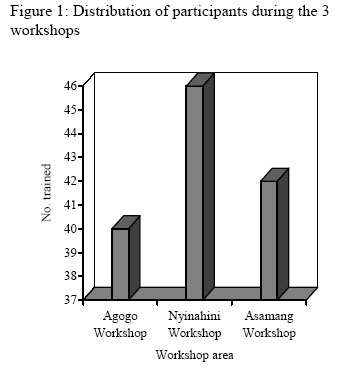
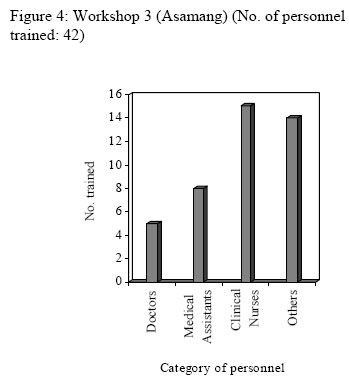
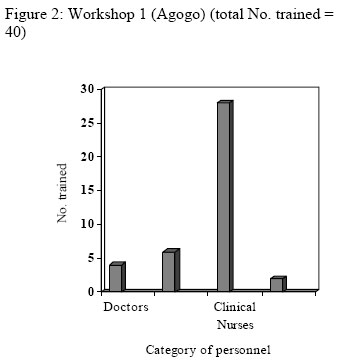
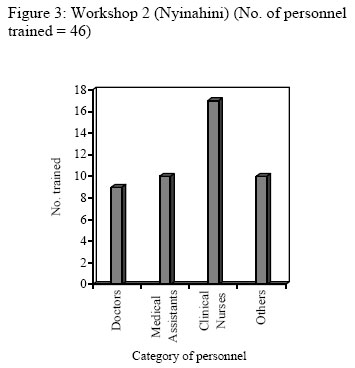
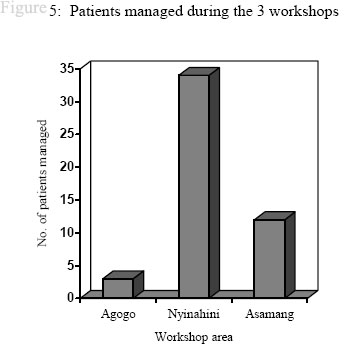
Methods The course was designed for district/community level health practitioners. The trainees included doctors, medical assistants, anaesthetists, clinical nurses and other health care providers in the districts. Each workshop was actually planned to have trainees selected from 1-3 nearby districts, all totaling 25 personnel. (But the reality was differen Figures 1 and 4). The training team (trainers), headed by a Consultant Plastic Surgeon (the Course Director) was coordinated by the Ashanti Regional Leprosy Control Officer. The team comprised of plastic surgeon 1, general surgeon 1, plastic surgical resident 1, clinical nurses 3, health educator 1 and anaesthetists 2. The course curriculum is shown in table 1. Results Within the period of 1 year (November 2001 till October 2002) 3 of such training workshops were held in 3 hospitals in 3 different districts in the region with participation from 15 hospitals/health centers drawn from 7 districts of the Ashanti Region. A total of 128 personnel were trained during the three workshops (Figures 1, 2, 3, and 4); Doctors 18, medical assistants 24, clinical nurses 60, others 26 (these were disease control officers and ward assistants). A total of 49 patients were treated during the three workshops (Figure 5). Table 1: Course curriculum
The course was a full, 2-day intensive workshop Discussion To measure the impact of these training workshops one needs to use some parameters such as:
In the absence of these data it would be difficult to measure the impact. Comparing these figures to the general case reports of BU in the Ashanti Region (which is on the increase) one can deduce that the majority of the patients are now receiving treatments at the district/community health institutions. This is confirmed by monitoring and evaluating visits to some of these hospitals. For example the doctors at Nkawie and Nyinahini Government Hospitals now do more surgery on Buruli ulcer patients. In the past (before the workshops) these hospitals did mainly wound dressings for these patients for a few days and then referred them to KATH. At the end of the five-year period of the running of the workshops, by which period the whole Ashanti Region would have been covered, there would be a proper assessment of the effectiveness of the workshops. The idea of Buruli Ulcer Management Teams (BUMTs) now exists “loosely” in most of the hospital/health centres where personnel had been trained at the workshops. Active BUMTs now exist in 6 health institutions. The Ghana Health Service needs to provide more surgical consumables to these health institutions in order to enable them manage these patients more effectively. As a result of these workshops active Buruli Ulcer Management Teams (BUMTs) have been formed in 6 health institutions in the region. Acknowledgement We thank the Ministry of Health/Ghana Health Service and the American Leprosy Missions for their help. We also appreciate suggestions and comments of participants, which enabled us to improve on subsequent workshops. References
Copyright 2005 - Annals of African Medicine |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}