 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
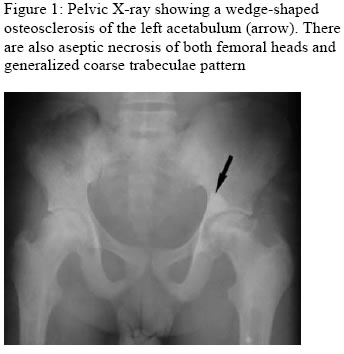
Annals of African Medicine, Vol. 4, No. 2, June, 2005, pp. 91-92 LETTER TO THE EDITOR AN UNUSUAL BONE INFARCT IN A YOUNG ADULT SICKLER E. N. Obikili, U. Okoye and B. C. Jiburum Department of Radiation Medicine, University of Nigeria Teaching Hospital, Enugu, Nigeria E-mail: okoyeij@infoweb.abs.net, unradiol@yahoo.com Code Number: am05022 Dear Editor Radiological features of sickle cell disease are multisystem and ubiquitous. The skeletal system is a frequent target of the consequences of sickling. One report has been shown that bone pain is the most common reason for admission to hospital. Bone infarcts, osteomyelitis, bone marrow necrosis and aseptic necrosis are common complications of sickle cell disease.2 This is a report of an unusual bone infarct in a sickler. The patient is 27-year-old known sickle cell patient who had been attending sickle cell clinic fairly regularly. On a number of occasions he was admitted and treated when he was in bone pain crises. Three years prior to presentation he started having a pain at the left hip joint. The pain was dull in character and was aggravated by prolonged walking or after sitting down for a long time. Later the right hip joint was also involved. The pain was relieved with analgesics. The patient later developed ulcer in the right leg. He was also treated for peptic ulcer. On examination he looked ill and pale, and walked with a limp. He weighed only 46kg for a height of 169cm. The laboratory investigations showed fetal haemoglobin of 10%, PCV of 20% and genotype of HbSS. Plain x-ray of the pelvis showed a wedge-shaped osteosclerosis of the left acetabulum in addition to the usual osseous findings in sickle cell disease: generalized coarse trabeculae pattern, aseptic necrosis of the femoral head, bone-within-bone appearance of the femora and reduction in the height of vertebral bodies. The abdominal ultrasound did not show the spleen. Autosplenectomy was therefore diagnosed. The other viscera appeared normal. Patients with sickle cell anaemia are prone to both infarctive and infective crises. Bone infarction is, however, the hallmark of sickle cell disease. Bones commonly involved include metaphysis and subchondrium of long bones, vertebral end-plates, and the heads of femur and humerus.3 Bone infarction may also cause local areas of bone sclerosis. The generalized skeletal features our patient had included osteoporosis, biconcave vertebrae, coarse trabeculae, bone-within-bone appearances, and fragmentation of the femoral heads. In addition to these, he also had a wedge-shaped osteosclerosis of the left acetabulum. The fact that it is not bilateral differentiates it from bone dysplasia. The wedge shape suggests that it is vascular in nature. Bone island, which is a differential, is uniformly dense, round or oval and usually has radiating thorn-like spicules.4 Bone infarctions are sometimes difficult to distinguish from osteomyelitis on plain radiographs. Different imaging modalities can be used to differentiate between the two. Scintigraphy will show areas of increased uptake in osteomyelitis and decreased uptake in acute bone infarctions. Ultrasonography will demonstrate subperiosteal tissue collection that may be associated with osteomyelitis. Ultrasound-guided aspiration is also useful in distinguishing abscess of osteomyelitis from haematoma due to bone infarction. Splenic infarction is relatively common in patients with sickle cell disease. Autosplenectomy may result from splenic infarctions.3 Our patient had autosplenectomy. The chronic leg ulcers, which our patient had, are known complications of sickle cell disease. Chronic leg ulcers result from vaso-occlusive complications associated with the decreased oxygen-carrying capacity of haemoglobin in patients with sickle cell disease or its variant5. It is important to be wary of infarctions in such atypical sites as a differential diagnosis of painful hip joint in sicklers. References
Copyright 2005 - Annals of African Medicine The following images related to this document are available:Photo images[am05022f1.jpg] |
| |||||||||

{kind=link}