 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
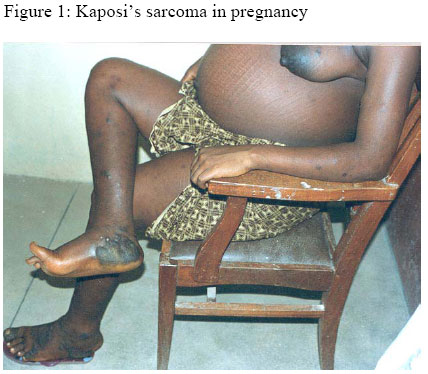
Annals of African Medicine, Vol. 4, No. 3, 2005, pp. 139-140 Images in Clinical Practice KAPOSI’S SARCOMA IN PREGNANCY M. S. Zayyam Department of Obstetrics and
Gynaecology, Ahmadu Bello University Teaching Hospital, Kaduna, Nigeria. A 28 year old woman with parity of 1+1 presented with painful bilateral leg swellings, rashes and discolouration of the skin of the legs of two months duration. She was 8 months pregnant. The abortion she had was spontaneous and was complicated by haemorrhagic shock requiring blood transfusion. She had a normal delivery the following year. The husband was a healthy 32 year old who had never had a blood transfusion. She weighed 65kg, was 1.6m tall and was had mild pallor. Temperature was 37o C. There was no pperipheral lymph node enlargement. There were dark brown patchy discrete raised, firm and non-tender lesions on both feet and legs. Ssimilar lesions were also present on the thighs and lateral aspects of the upper limbs; the ttrunk, abdomen were relatively spared (Figure 1). The abdomen was distended; the symphysio-fundal height was 42cm and multiple foetal poles were felt. No other masses were felt in the abdomen. The twin foetuses were both in cephalic presentation. Examination of the chest was normal. Haemogram was 10g/dl, white cell count 6.4 x 109/ll, neutrophils 70%, lymphocytes 22% and eosinophils 8%. The CD4 counts was 210/ul but dropped to 205/ul within one week. VDRL test was negative. Chest radiograph was normal and stool was negative for occult blood. Serum electrolytes and urea and liver function tests were normal. Biopsy of lesions confirmed Kaposi’s sarcoma. The patient’s serum was positive for HIV (confirmed by Western blot). The husband was HIV sero-negative (repeated twice at 6 month intervals). The surviving child was also HIV sero-negative. She was managed with analgesics and prophylactic antibiotics in view of the low CD4 count. Despite extensive counseling on the need to reduce the risk of transmission to the babies with elective caesarean section and use of antiretroviral drugs, the patient opted for vaginal delivery and could not afford antiretroviral therapy. She had a spontaneous twin delivery of live fetuses at 39 weeks gestation. The first twin weighed 3.5 kg and second twin 3.2 Kg. Both babies tested positive to HIV 1 and remained positive. The disease ran an aggressive resulting in death six months postpartum. Kaposi's sarcoma (KS) is an opportunistic tumor that develops with increased frequency (100,000-fold) after HIV infection. 1 It characteristically presents in HIV seropositive homosexual or bisexual men. It is r rare in women.2KS is very rare in pregnancy.3 - 5 The incidence of various types of KS in men and women are shown on table 1. The reason for these differential rates has been ascribed to human chorionic gonadotropin (hCG) or hCG-like hormone, notably luetenizing hormone. 6 The evidence supporting the effect of hCG on KS has been confirmed in experimental studies using mice where pregnant mice were protected and apoptosis was induced in Kaposi's sarcoma cells by preparations of hCG both in vitro and in vivo.7,8 Table 1: Incidence of various types of Kaposi’s sarcoma in males and females
That KS runs an aggressive natural course in twin pregnancy further cast’s doubt to the anti- KS effect of hCG as such a pregnancy is expected to confer a relative protection. The progressive unraveling of the KS pathogenesis, with subsequent isolation of human herpes virus 8 or KSHV has lead to the establishment of reliable linkage with the tumor and development of novel therapeutic approaches. 9,10It would have been interesting to establish the serological status for HHV8 for this patient and the twins as mother-to child transmission for the virus has also been confirmed with reports of KS in neonates. 11, 12 Reference
Copyright 2005 - Annals of African Medicine
The following images related to this document are available:Photo images[am05035f1.jpg] | |||||||||||||||||||||||
| |||||||||

{kind=link}