 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 4, No. 4, 2005, pp.180-182 AMYLOID GOITRE FOLLOWING CHRONIC OSTEOMYELITIS: CASE REPORT AND REVIEW OF LITERATURE 1A. Z. Mohammed, 2S. T. Edino and 1O. Ochicha Departments of 1Pathology
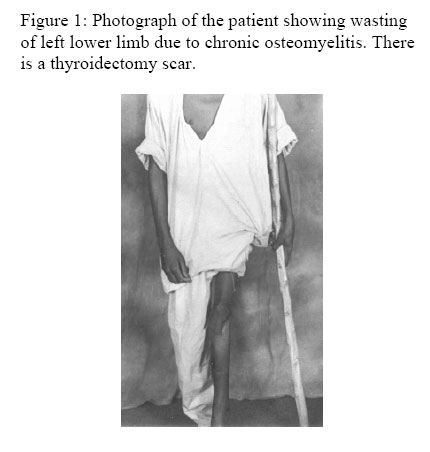
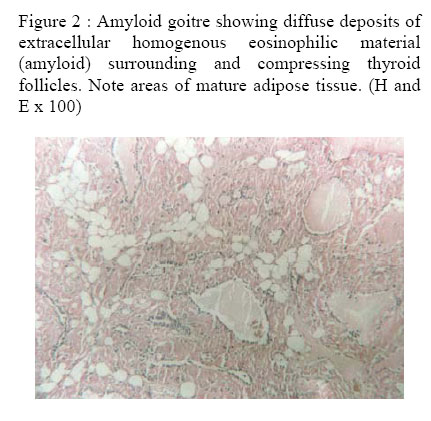
and 2Surgery, BayeroUniversity, Kano, Nigeria Code Number: am05045 Abstract Amyloid Goitre is a rare clinical entity associated with systemic amyloidosis. It poses a significant diagnostic and therapeutic challenge and may be confused with a neoplastic goiter. We present the case of a 20 year old male patient who presented with a rapidly enlarging goiter, several years after resolution of chronic osteomyelitis. Histologic examination of the thyroidectomy specimen showed extracellular deposits of congophilic amyloid diagnostic of amyloid goitre. Similar cases in the literature are reviewed. Key words: Amyloid goitre, thyroidectomy, osteomyelitis Résumé Le goitre amyloïde est une entité clinique rare associée à une amylase systémique. Il pose un problème diagnostic et thérapeutique important et peut causer une confusion avec un goitre néoplasique. Nous rapportons le cas d’un homme de 20 ans qui avait consulté pour un goitre d’augmentation rapide de volume, plusieurs années après la résolution d’une ostéomyélite chronique. L’examen histologique de la pièce de thyroïdectomie a montré des dépôts extracellulaires congophyles amyloïdes, posant le diagnostic de goitre amyloïde. Des cas similaires dans la littérature ont été revus. Mots clés : Goitre amyloïde, thyroïdectomie, ostéomyélite Introduction Amyloid goitre (AG) is a rare clinical entity characterized by microscopic infiltration of the thyroid gland by amyloid material.1 It is encountered in the setting of primary or secondary systemic amyloidosis where it is frequently asymptomatic. Only rarely does thyroid amyloidosis result in a clinically palpable goiter.2 Preoperative diagnosis may prove difficult and the condition can be confused easily with a neoplastic goitre both clinically and cytologically.3 Inspite of extensive infiltration of the thyroid by amyloid deposits, thyroid function usually remains normal.2,4 Case report A 20 year old male student was referred to the surgical outpatient clinic of Aminu Kano Teaching Hospital with a 2 year history of a progressively enlarging neck mass. The mass was painless and had recently caused him some dysphagia. There was however no voice change. He had suffered from chronic osteomyelitis of the left lower limb for seven years which had been treated with cyclical broad spectrum antibiotics before resolving spontaneously 5 years prior to presentation. Physical examination showed grade 3 finger clubbing and scanty silky scalp hair (Figure 1). A 16cm x 10cm diffuse multinodular goitre was present in the neck but no clinical signs of thyroid dysfunction were evident. There was marked atrophy and weakness of the left lower limb, and several puckered scars were noted on the limb. He also had a limping gait. Examination of the respiratory and cardiovascular systems were normal and abdominal organs were not palpably enlarged. Complete blood count, serum urea, creatinine, electrolytes, calcium and phosphate were within normal reference values. There was decreased serum albumin level (27.5g/l) and proteinuria of 0.5g/L. Haemoglobin genotype was AA by electrophoresis. Tests of thyroid function showed T3 of 1.47 nmol/L, T4 of 57.38 nmol/L and thyroid stimulating hormone of 1.08 µiu/ml. A fine needle aspiration biopsy demonstrated features of a benign follicular neoplasm. Indirect laryngoscopy showed normal vocal cords and an X-ray of the neck showed tracheal deviation to the left side, but no calcifications were visualized. At surgery the thyroid gland was found to be uniformly diseased and friable raising the suspicion of malignancy. Since facilities for frozen section are not available, a total thyroidectomy was done, with levothyroxine supplementation (0.3mg daily). The postoperative state was uneventful. The thyroidectomy specimen was friable, measured 14 x 8 x 5.5cm and weighed 260g. The cut surface was variegated and showed grey tan solid areas and dark brown areas. Microscopy showed diffuse deposits of amyloid surrounding compressed thyroid follicles (Figure 2). There were areas of mature adipose tissue, lymphocytic infiltrates and foreign body giant cell reaction. The amyloid demonstrated positive staining with Congo Red which was bleached by potassium permanganate. The patient was discharged home on the seventh postoperative day on levo -thyroxine supplementation for life and has remained well at one year of follow up. Discussion The present case illustrates the diagnostic and therapeutic challenges encountered in the management of AG. Affected patients are usually adults between the age of 23 and 75 years, and most series show a predominance of males over females.5,6 Subclinical deposits of amyloid in the thyroid are more common than symptomatic disease, and diagnosis is only first achieved at autopsy in some cases.2,5 Rarely, patients present with a progressive or rapidly enlarging goiter that is unaffected by administration of levothyroxine.4,7 AG may mimic a malignant goiter when symptoms of compression like dysphagia, dyspnoea and hoarseness appear.2,5 Clinical evidence of thyroid dysfunction is however uncommon even with diffuse infiltration of the gland by amyloid deposits, and is mainly in form of hypothyroidism.2,4 An occasional case of AG may be detected in a background of thyrotoxicosis.8 Additional features of systemic amyloid deposition when present include macroglossia, hepatomegaly, splenomegaly, cardiac failure and renal impairment. A high index of suspicion is therefore necessary for diagnosis, which is made easier where a background history of a recognized cause of amyloidosis exists as is the case in this report. Fine needle aspiration biopsy (FNAB) facilitates the preoperative diagnosis of AG and helps distinguish it from other types of goitres and from malignancy.3,5,8 The aspirated material can be stained with Congo Red to demonstrate amyloid, but attention needs to be paid to the morphology of the cells accompanying amyloid to allow distinction from medullary carcinoma of the thyroid, another important cause of amyloid deposits in the thyroid. Difficulties in obtaining adequate aspirates in some cases poses limitations to FNAB diagnosis.7 In such situations, a core needle biopsy or open surgical biopsy aids in preoperative diagnosis, even though it may be complicated by haemorrhage. Histologic diagnosis of biopsy specimens rests on the demonstration of extracellular deposits of amyloid in a nodular or diffuse pattern around compressed thyroid follicles. Areas of mature adipose tissue, lymphocytic infiltrates and giant cells may also be present.5 Diagnosis is confirmed by positive histochemical staining of amyloid with congo red and bleaching following treatment with potassium permanganate. Immunohistochemistry and electron microscopy provide additional diagnostic tools to determine the nature of the amyloid proteins.9 Treatment is directed at treating the specific type of amyloidosis, controlling any form of thyroid dysfunction and the local thyroid enlargement. Thyroidectomy either total or subtotal is commonly performed with levothyroxine supplementation. The prognosis is generally poor in patients with primary amyloidosis because of progression to renal failure. AG secondary to chronic infections is associated with better prognosis and long term survival.6 In this report, lack of initial clinical suspicion prevented a preoperative diagnosis in spite of an appropriate clinical background, which would have necessitated further evaluation of FNAB specimen with congo red stains. A plea is therefore made for clinicians particularly in developing countries, where chronic infections are still prevalent to recognize this condition when it presents. Our patient is still being followed up at the surgical outpatient clinic, and has remained well two years post thyroidectomy. Particular attention is however placed on regular monitoring of renal function and thyroid hormonal status. Acknowledgement We are grateful to Mallam Ibrahim Lawal of the Medical Illustration Unit, Faculty of Medicine, Bayero University Kano for the photographs. References
Copyright 2005 - Annals of African Medicine The following images related to this document are available:Photo images[am05045f2.jpg] [am05045f1.jpg] |
| |||||||||

{kind=link}
{kind=link}