 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 5, No. 1, 2006, pp. 10-15 Peak Expiratory Flow Rate in Normal Hausa-Fulani Children and Adolescents of Northern Nigeria 1F. B. O. Mojiminiyi, 1U. V. Igbokwe, 2O. P. Ajagbonna, 3S. I. Jaja, 3R. R. Ettarh,4R. U. Okolo, 2U. E. Mojiminiyi and 1A. Gambo Departments of 1Physiology, 2Veterinary Physiology and Pharmacology, 4Anatomy, Usman DanFodio University, Sokoto, Nigeria and 3Department of Physiology4, College of Medicine, University of Lagos, Nigeria Reprint request to: Dr. F. B. O. Mojiminiyi, Department of Physiology, College of Health Sciences, UsmanDanFodioUniversity, P. M.B. 2254, Sokoto, Nigeria. E-mail: mojiminiyi@yahoo.co.uk Code Number: am06003 Abstract Background: Peak expiratory flow rate (PEFR) is a useful
parameter for assessing respiratory function in health and disease. However
there are few studies reporting normal values of this parameter in Northern Nigeria in general and the North western zone in particular.
Also prediction formulae for predicting PEFR from anthropometric parameters are
not available for this population. The present study was therefore designed to
measure Peak expiratory flow rate (PEFR) in normal Hausa-Fulani children and
adolescents in Sokoto and to derive prediction formulae for this population. Key Words: Peak expiratory flow rate, Hausa-Fulani, prediction formulae Résumé Fond
: Le débit expiratoire maximal (DEM)
est un paramètre utile pour évaluer la fonction respiratoire dans la santé et
la maladie. Cependant, il y a peu d'études indiquant des valeurs normales de ce
paramètre au nord du Nigéria en général et la zone occidentale du nord en
particulier. En outre les formules de prévision pour prévoir le DEM des
paramètres anthropométriques ne sont pas disponibles pour cette population. La
présente étude a été donc conçue pour mesurer le débit expiratoire maximal
(DEM) dans les enfants et les adolescents normaux de hausa-Fulani-Fulani à
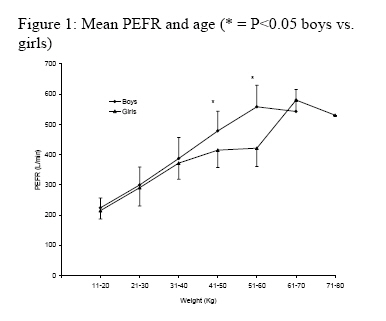
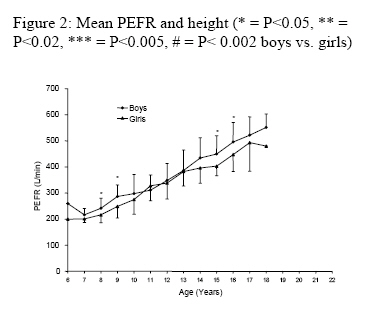
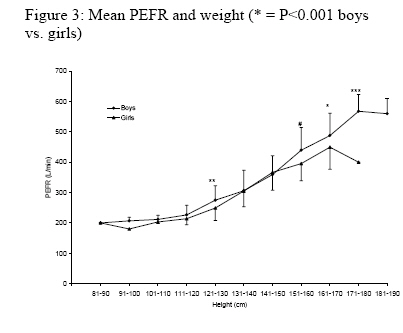
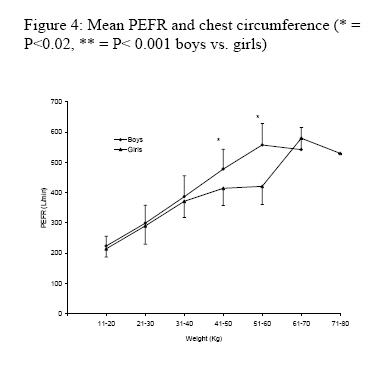
Sokoto et pour dériver des formules de prévision à cette population. Mots clés : Débit expiratoire maximal, Hausa-Fulani-Fulani, formules de prévision Introduction Peak expiratory flow rate (PEFR) is a useful parameter for assessing patients with obstructive airway disorders.1 By virtue of its simplicity of measurement and its positive correlation with spirometric parameters such as forced vital capacity and forced expiratory volume in one second, it has been suggested that it be used in the assessment of respiratory function particularly in children who may not be able to follow instructions required for spirometric measurements.1 A number of studies on PEFR have been carried out in Nigerian children1, 2, 4 and adults. 5-8 However these studies have been limited largely to the South-Western zone of Nigeria whose ethnic composition is predominantly Yoruba. Since PEFR is affected by anthropometric factors such as height, weight, body surface area, age and chest circumference 1,4-8 which tend to be different in different ethnic groups it will interesting to measure this parameter in other ethnic groups in Nigeria. One study has reported the measurement of PEFR in Hausa adolescents of Northern Nigeria. 3 This is a report to establish the normal PEFR values for Hausa-Fulani children and adolescents in Sokoto, Nigeria. Materials and Methods Six hundred and sixteen Hausa-FulaniSchool children and adolescents, 376 boys and 240 girls, aged between 6 and 18 years were randomly selected from two primary and two secondary schools in the Sokoto metropolis. These schools were chosen because they were attended by children and adolescents that cut across the socio-economic groups in Sokoto. The children and adolescents recruited were apparently healthy and did not smoke cigarettes nor had a history of smoking cigarettes in the past. Subjects with history of chronic cough or respiratory disease, cardiac or systemic disease, or chest deformity were excluded from the study. Anthropometric data obtained subjects included age, height without shoes, weight with minimal clothing and without shoes and chest circumference. Height was measured using a scale carefully marked out on the wall using a metre rule. Weight was measured using a bathroom scale. Chest circumference was measured using an inelastic tape rule during expiration at the level of the fourth intercostal space.6 PEFR was obtained from our subjects in the standing position using the mini-Wright peak flow meter (Airmed, London, England). The measurement of the PEFR was demonstrated before the children and adolescents to show them how it was done. Then they were instructed to inspire maximally, close their mouths tightly around the meter's mouthpiece and expire as maximally and as forcefully and quickly as possible. PEFR measurements were obtained at ambient temperature and pressure saturated with water vapour (ATPS). Two practice attempts were first made in each volunteer. Those that could not follow the instructions or perform the test well were excluded. Three measurements were then obtained consecutively from those subjects that performed the test well at about two minute intervals. The highest of these three measurements was recorded. Measurement of anthropometric parameters and PEFR were carried out in such a way that each member of the team performed a particular measurement e.g. one person measured the height while another PEFR. The use of one observer per measurement was maintained throughout the study. The leader of the team (FBOM) randomly repeated some of the measurements to validate their accuracy. The measured variables are presented as mean ± SD (standard deviation). The PEFR and the various anthropometric parameters measured were compared between the boys and girls using unpaired t test. PEFR was also correlated with the anthropometric parameters and prediction formulae derived for predicting PEFR from the anthropometric parameters obtained in the present study. The observed PEFR values obtained in the present study were compared with values obtained using prediction formulae derived in other Nigerian populations using paired t test. P < 0.05 was taken as statistically significant. Results Table 1 presents a summary of the mean values of the anthropometric parameters and PEFR obtained in this study. The boys were significantly older (P < 0.001), taller (P < 0.001), heavier (P < 0.01) and had higher PEFR (P < 0.001) than the girls. However the chest circumference showed no significant difference between the sexes. Table 2 shows the correlation coefficients (r) between PEFR and the anthropometric parameters measured in this study. In boys PEFR correlated most with weight followed by age, height and then chest circumference. In girls, PEFR correlated most with height, followed by weight, chest circumference and age. Figure 1 shows the relationship between PEFR and age. In our subjects PEFR increased with age. PEFR remained similar in both sexes at most ages except at ages 8, 9, 15 and 16 where PEFR was significantly higher in boys than in girls (P < 0.05 respectively). Figure 2 illustrates the relationship between PEFR and height. PEFR increased with height. PEFR did not differ significantly between the boys and girls at the same height intervals except at height intervals 121-130 cm (P < 0.02), 151-160 cm (P < 0.002), 161-170 cm (P < 0.05) and 171-180 cm (P < 0.005) where PEFR was significantly higher in boys than in girls. Figure 3 shows the relationship between PEFR and weight. PEFR increased with weight. PEFR showed no significant difference between the sexes at most weight intervals except at weight intervals 41-50 and 51-60 kg where PEFR became significantly higher in boys than in girls (P < 0.001 respectively). Presented in Figure 4 is the relationship between PEFR and chest circumference. PEFR increased as chest circumference increased. The sex difference in PEFR did not show at a chest circumference interval of 61-70 cm. However at other chest circumference intervals i.e. 51-60 cm (P < 0.02), 71-80 cm (P < 0.001) and 81-90 cm (P < 0.001) the PEFR was significantly higher in boys than in girls. Regression analyses were carried out (Table 3) on the relationship between PEFR and each anthropometric parameter measured in order to obtain formulae for predicting PEFR from each anthropometric parameter. The formulae chosen were those that had the least standard error of estimates4 (S.E.E.). In boys weight had the least S.E.E. and in girls, age had the least S.E.E. Regression equations using only one anthropometric parameter were chosen because using multiple anthropometric parameters (i.e. multiple regression analyses) did not enhance the predicting power of the formulae nor lower the S.E.E. The prediction formulae obtained in this study were; Boys: PEFR (L/min) = 85.83 + 8.25 x weight (kg) (± 3.15); Girls: PEFR (L/min) = 3.67 + 28.15 x age (years) (± 3.51) Tables 4 and 5 show a comparison of observed PEFR in children of specific ages with predicted PEFR using equations derived from Nigerian populations by earlier workers. In males the predicted values were significantly lower than the observed values at each age except the predicted value obtained using the formula of Aderele and Oduwole (1983)2 at age 8 which was not significantly different from the observed value (Table 4). In females, whilst the observed and predicted PEFR remained similar at age 8, the predicted PEFRs were significantly lower than the observed at ages 12 and 16 years respectively (Table 5). Table 1: Summary of anthropometric parameters and PEFR obtained in the present study. NS = Not significant
NS: Not significant; PEFR: Peak expiratory flow rate Table 2: Correlation coefficients (r) between PEFR and various anthropometric parameters
Table 3: Coefficients for predicting PEFR from age, weight (wt), height (ht) and chest circumference (cc)
S.E.E.: Standard error of estimates; *: Least S.E.E. for girls; **: least S.E.E. for boys Table 4: Comparison of observed and predicted PEFR in various ages in males
Results are expressed as mean ± SD.NS: Not significant Table 5: Comparison of observed and predicted PEFR in various ages in females
Results are
expressed as mean ± SD.NS: Not significant Discussion In this study, it was observed that the mean PEFR was significantly higher in boys than in girls. In this study also, it was observed that PEFR correlated positively with age, height, weight and chest circumference. Thus the higher PEFR in the boys compared to the girls could be due to the fact that they were significantly older, taller and heavier (table 1). Chest circumference also seems to contribute to this sex difference in PEFR. Although chest circumference seemed to be similar in boys and girls when the results were pooled together (table 1), the boys tended to have higher PEFRs than the girls within similar ranges of chest circumference (Figure 4). The higher PEFR observed in boys compared to girls is similar to earlier findings in Nigerians1, 3 but different from others.2, 4 The latter workers generally reported a similar PEFR in both sexes except at certain ages. PEFR correlated positively and significantly with all anthropometric parameters measured in either sex. This is generally in agreement with the findings of earlier workers in Nigerian children.1-4 However in the present study PEFR correlated best with weight in boys and best with height in girls. Variable results have been obtained as regards which anthropometric parameter correlates best with PEFR among Nigerian children of either sex. Thus while Aderele and Oduwole (1983)2 found that height had the highest correlation coefficient with PEFR in both sexes, Onadeko et al (1984)1 and Ali and Vahalia (1991)3 reported that weight correlated best with PEFR in boys and age in girls. Also Jaja and Fagbenro (1995)4 observed that body surface area in boys and age in girls correlated most with PEFR. Furthermore, although it has been reported that PEFR correlates more with height than weight among Caucasians9 most reports1, 3, 4 in Nigerian children suggest the opposite i.e. that PEFR correlates more with weight than with height. However the latter reports do not agree with the findings of Aderele and Oduwole (1983)2 that suggested that height correlated better with PEFR than weight in both sexes neither do they agree with the present findings that suggested that height correlated better with PEFR than weight in girls. The reason for this difference is not clear but may be due to peculiarities of the populations studied or differences in methodology. Also the observed PEFR in this study was compared with predicted values using prediction equations derived previously among populations of children in Ibadan, Nigeria whose ethnic composition is predominantly Yoruba1, 2 and in the cosmopolitan city of Lagos4 both in South-Western Nigeria. To the best of our knowledge prediction equations from other zones are lacking particularly among the Hausa-Fulani of Northern Nigeria. Prediction equations derived among Caucasian children were not used because it is already established that they poorly predict respiratory indices in Nigerians.1, 7, 10, 11 In males only the formula of Aderele and Oduwole (1983)2 correctly predicted the PEFR of the population of children and adolescents in this study and only at age 8. At other ages this formula failed to correctly predict the observed PEFR. Since this formula is height-based this finding may suggest that the population of Hausa-Fulani children that are 8 years old in this study are similar in height to the population of Yoruba children studied by Aderele and Oduwole (1983)2 in spite of differences in ethnic group while at other ages they are dissimilar. The other prediction equations (Onadeko et al, 19841 and Jaja and Fagbenro 1995)4 used to predict PEFR values in males gave results that were significantly different from observed values suggesting that the populations from which they were derived are dissimilar to the population in the present study. In females at age 8 both formulae used correctly approximated the observed PEFR (table 5). Since both formulae are based on height this suggests that the female children of age 8 were identical in terms of height in the present study compared to the populations from which those prediction formulae were derived in spite of ethnic differences. At the other ages (12 and 16 years) the prediction equations failed to correctly predict the observed values suggesting that at these ages the populations had become dissimilar. Taken together the above findings may suggest that the anthropometric features upon which the prediction formulae were based may or may not be similar in Nigerian children from different ethnic groups at age 8 or in pre-pubertal years whilst they differed significantly in the pubertal (12 and 16) years. Also these findings support the notion that the usefulness of prediction equations may be limited to the population or ethnic group from which they were derived. Thus no single prediction equation can serve the diverse and huge population of Nigeria. It also underscores the need for actual measurements of PEFR and other respiratory indices to be done for each locality. Normal PEFR values have been obtained in normal healthy Hausa-Fulani children and adolescents in Sokoto and prediction equations derived for use among them. It is concluded that actual PEFR measurements should be done for each ethnic group or locality and the usefulness of prediction equations may be limited to the ethnic group or locality from which they were derived. Acknowledgements We are grateful to the children and adolescents who volunteered for this study. We are also grateful to the Headmasters/Principals of the following Schools: Usman DanFodio University Primary School, Mohammed Zakko Modern Primary School, Sultan Bello College and Nana Girls Day Secondary School all in Sokoto, for giving us access to their Students. References
The following images related to this document are available:Photo images[am06003f3.jpg] [am06003t3.jpg] [am06003f4.jpg] [am06003f2.jpg] [am06003f1.jpg] [am06003t2.jpg] [am06003t1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}