 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
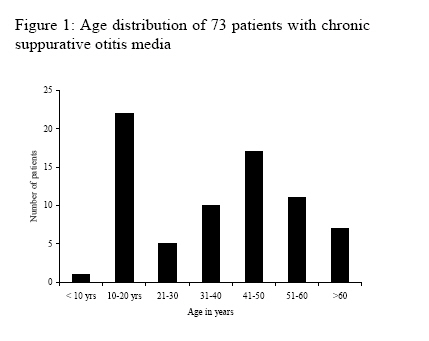
Annals of African Medicine, Vol. 5, No. 1, 2006, pp. 24-27 Surgical Management of Chronic Suppurative Otitis Media: A 3-year Experience M. A. Yaor, A. El-Kholy and B. Jafari Department of Ear, Nose and throat, Trafford GeneralHospital, Manchester, UK Reprint requests to: Mr M. A. Yaor, Department of Ear, Nose and Throat, Trafford GeneralHospital, Moorside Road, Davyhulme, Manchester. M41 5SL, U.K. E-mail: mosesayaor7@aol.com Code Number: am06006 Abstract Background/Objective:To determine the outcome of surgery for chronic
suppurative otitis media at our department over 3 years, between 2001 and 2003.
The outcome measures were; achievement of dry ear, closure of tympanic membrane
perforation and improvement in hearing for patients who had myringoplasty. Key words: Cholesteatoma, non-cholesteatomatous otitis media, tympanoplasty, surgery, outcome Résumé Fond/Objectif: Pour déterminer les résultats de la chirurgie pour
l’otite moyenne chronique suppurative à notre département pendand une période
de 3 ans, entre 2001 et 2003. Les mesures de résultats étaient; accomplissement
d'oreille sèche, fermeture de perforation de tympan secondaire et amélioration
d’audition pour les malades qui ont eu la myringoplastie. Mots clés: Cholestéatome, otite moyenne non-cholestéatome, tympanoplastie, chirurgie, résultats Introduction Chronic suppurative otitis media (CSOM) with or without cholesteatoma is a persistent disease, which can cause severe destruction of the middle ear and mastoid and lead to irreversible sequelae. In the present antibiotic era, the complications are rarely seen. Surgery plays an important role in its management and the outcome measures are closure of tympanic membrane perforation in myringoplasty, eradication of disease and achievement of a dry and safe ear in mastoidectomy and in some cases, improvement of hearing where ossicular reconstruction or ossiculoplasty is also carried out. The aim of this retrospective study was to evaluate our results of surgeries performed in patients with CSOM at our hospital over a three year period and a review of literature. Materials and Methods A proforma was designed to retrospectively collect data on 73 patients who had surgery for chronic suppurative otitis media (cholesteatoma and non cholesteatomatous disease) in the ENT department at Trafford general hospital, Manchester between January 2001 and December 2003. There were 41 males and 32 females, aged 9 - 84 years (mean o37 years); 17 were children aged 9 to 15 years (Figure 1). Twenty five patients had cholesteatoma which was limited to the middle ear and mastoid, 48 patients had non-choleateatomatous, tubo-tympanic mucosal disease. Forty one primary myringoplasties were performed with 6 revisions, 2 had tympanomastoidectomy. Twenty nine mastoidectomies were carried out and all were canal wall down procedures with meatoplasties; 32 ears were wet at the time of surgery. Computed tomography (CT) scan of the temporal bone (mastoids) was performed for mastoidectomy patients. The commonest incision was the post-auricular, others were enaural and permeatal. Facial nerve monitor was used in all the mastoidectomies and patients were covered with prophylactic antibiotics post-operatively. Patients were followed up for up to 18 months. Results Closure of tympanic membrane perforation was achieved in 89% over all and the rate in children 9 – 15 years was 90%. These rates are comparable to those in literature, which varies from 66.6% to 93%. Site and size of the perforations were not assessed in this study, so their effect on the outcome could not be assessed. Three patients had discharging ears at the time of surgery, 2 of them had persistent perforation 6 months after surgery. Two patients with non-cholesteatomatous disease had tympanomastoi-dectomy and their ears were dry and tympanic membranes were intact at over 6months follow up. Otorrhoea was reduced from a pre-operative rate of 43% (n=32) over all to 15% (n=11). 29 (90.6%) mastoids were wet at the time of surgery, and post-operatively, 9 (28%) were active, giving a success in achieving a dry ear of 62.5% (n=20). Forty one patients had myringoplasty, but pre and post-operative audiometric results were available in 37 of them (Table 1). Hearing was improved in all, binaural hearing was achieved in 6 patients and in 4 patients, the operated ear became the better ear. Air-bone gap was closed to within 10dB in 26 (78.3%). One patient presented with acute mastoiditis with facial nerve palsy, House Brachman grade 2, which got worse after the surgery to grade 4, but improved to grade 2-3 at 9 months follow up. There were no other complications in this study population. Table 1: Post-operative air-bone gaps in 37 patients undergoing myringotomy
Discussion Chronic suppurative otitis media and cholesteatoma is said to a vanishing disease among western populations, with the incidence of new cases declining, Alho OP, et al (1997). 1 We still continue to see new cases in both adults and children. In this study, of the 29 mastoidectomies, only 6 were revisions and 25 (86.2%) were cholesteatomas, 7 of them were in children 9-15 years of age. The mastoidectomy audit by the Royal college of Surgeons of England2 reported 320 out of 611 mastoidectomies were primary procedures performed for cholesteatoma in 1991 by 54 consultants and an average number of patients per consultant for one year was 11, the average in this study is12 which is comparable and could indicate that the burden of chronic otitis media has not changed much over 9-12 years. Our success rate in closing tympanic membrane perforations was 89%, which is comparable to the rates quoted in literature, which are between 66.6% 3 and 93%.4 The 17 children in our study were aged 9 – 15 years, 10 had myringoplasty and the success rate in closure of perforation among them was 90%. Umapathy et al 5 reported 90% closure of perforation in 100 consecutive children aged 4-14 years. Our rate is comparable but the study population is smaller and the study design and criteria for success are not similar, therefore, comparison is weak. However, it shows that a success rate in children is high and comparable to that in adults. The state of the middle ear did influence the outcome of myringoplasty in our study. 3 ears were wet at the time of surgery and 2 failed (66.7%), however there is controversy regarding the outcome of tympanoplasty in operating on wet ears. Vartianem6 and Baylan7 say that, the state of the middle ear at the time of surgery does not affect graft take rate while Chan 8 is of the opinion that eradication of disease takes priority and precedes tympanic reconstruction and Gersdorff 9 suggest that it influences the surgical outcome, wet ears having a higher rate of re-perforation and suggests that such ears should have mastoidectomy as well. McGrew10 in their paper concluded that mastoidectomy impacts the clinical course of the disease in patients by reducing the number of patients requiring future surgery and the disease progression. Mishiro 11 in a retrospective study of 251 ears with non-cholesteatomatous chronic otitis media operated upon over 11 year period, concluded that mastoidectomy is not helpful in tympanoplasty for non-cholesteatomatous disease, even if the ear is discharging. However, this is a retrospective study and with its inherent drawbacks limits the validity of such a conclusion. 62.5% of the cavities (canal wall down) in this study were dry up to 12 months post-operative follow-up and 28% of were wet. The figures are comparable to those of the mastoidectomy audit by the RoyalCollege of surgeons of England 2 which reported 60% dry and 18% wet cavities at 3 and 15 months post-operatively for open cavity mastoidectomy. It is generally reported that open cavity or canal wall down mastoidectomy has a higher failure rate and poor disease control resulting in a significantly high proportion of wet ears post-operatively. Khalil12 in a study of the frequency of out patient visits, clinical problems at the visit and the percentage of discharged patients in 101 patients who had canal wall down mastoidectomy, concluded that open cavity carries an intrinsic morbidity resulting in long term attendance in the outpatient. Hearing results were assessed in the myringoplasty patients only and pre and post-operative audiograms were available in 37 of the 41 patients. Hearing improved in all, air-bone gap was closed to within 10dB in 78.3%, binaural hearing was achieved in 6 patients (16.2%) and in 4 patients (10.8%) the operated ear became the better ear. Chronic suppurrative otitis media with or without cholesteatoma is still present with us and management is still a challenge to Otolaryngologists. Surgery for chronic otitis media in both cholesteatoma and non-cholesteatomatous disease is highly successful in achieving a dry ear, closing the tympanic membrane perforation, preventing recurrence and improving hearing in both adults and children. Though improvement in hearing is not always a priority for patients undergoing tympanoplasty, from this study (though retrospective) and reports in literature, it is reasonable to include and inform patients of this outcome while consenting them for surgery. References
Copyright 2006 - Annals of African Medicine The following images related to this document are available:Photo images[am06006t1.jpg] [am06006f1.jpg] |
| |||||||||

{kind=link}