 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 5, No. 1, 2006, pp. 33-37 Characteristics of Craniofacial Trauma in a Rural Hospital in South India 1A. Agrawal, 2R. B. Prasad, 3L. Shetty, 4S. Nachiappan and 5M. Manju 1Department of Neurosurgery, K. S. Hegde Medical Academy, Mangalore, 2Department of Cranio-maxillofacial Surgery, Nitte Meenakshi Institute of Craniofacial Surgery, Mangalore, 3Department of Radiology, K. S. Hegde medical Academy, Mangalore, 4 Department of Maxillofacial Surgery, A.B. Shetty Memorial Institute of Dental Sciences, Mangalore and 5Department of Surgery, K. S. Hegde Medical Academy, Mangalore, India Reprint requests to: Dr. Amit Agrawal, Department of Neurosurgery, K.S.HegdeMedicalAcademy, Deralakatte-575018, Mangalore, Karnataka, India. E-mail: dramitagrawal@gmail.com Code Number: am06008 Abstract Background/Purpose:Purpose of
this study was to evaluate the population characteristics of patients with both
head injury and facial fractures in rural centre. Key words: Craniofacial trauma, neurological injury, facial injury, maxillofacial trauma Résumé Fond/But: Le but de cette étude était d'évaluer les
caractéristiques de population des malades avec les blessures
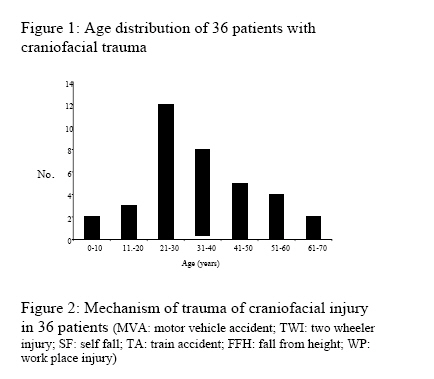
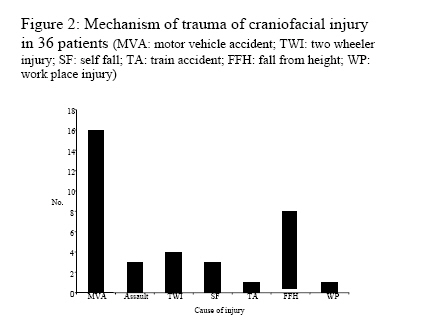
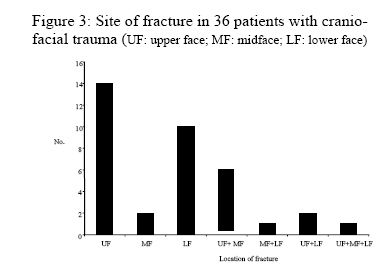
crâniens et les ruptures faciales au centre rural. Mots clés: Trauma crânio-facial, blessure neurologique, rupture facial, trauma maxillofacial Introduction Craniofacial trauma can involve both facial skeleton and skull with brain and its coverings. High velocity impacts may result in fracture of facial bones and life threatening intracranial hemorrhages in different compartments requiring urgent neurosurgical intervention. 1 - 4 However most of the time, patients with cranial and maxillofacial trauma will need a team approach including the maxillofacial surgeon. The purpose of this study was to analyze the characteristics of craniofacial fracture and neurological injuries in a rural hospital. Material and Methods This study was a retrospective review performed at JusticeK.S.HegdeCharitableHospital, Deralakatte (Mangalore). This is a hospital situated in coastal rural area of south India .The period of study was from March 2004 to February 2005. A total of 36 patients who sustained cranial and facial injuries were included in this study. Patients’ charts were reviewed and injuries were identified and analyzed according to age, sex, cause of injury, mechanism of injury, type and location of the facial injury and neurologic injuries. Appropriate skull X-Rays were done in all patients and patients with impaired consciousness, neurological signs or clinical signs of a basal skull fracture, an initial CT scan was also performed. Patients were considered to have a skull or facial fracture on the basis of a plain radiograph or a CT scan evaluated by a radiologist. Fractures of the facial skeleton based of facial bone imaging were grouped either alone or combination as follows: 1) Lower face (LF), which included the mandible; 2) Midface (MF), which included the maxilla, nose, zygoma, and orbits; and 3) Upper face (UF), which included the frontal bone. 5 Neurologic injuries ranged from loss of consciousness to depressed skull fracture requiring neurosurgical intervention. Brain trauma was handled by neurosurgery department and complex facial fractures were repaired by the Oral and Maxillofacial Surgery Department. Results Age and sex Thirty six patients were admitted with craniofacial trauma with a mean age of was 32.64 years (range 4 - 70 years). Majority of the patients (55.5%) were in 3rd and 4th decade of age (Figure-1). There were 35 males and one female. Cause of injury Most common cause of injury was motor vehicular accidents (44.4%) followed by fall from height (22.2%), particularly from coconut tree (16.6%). Assault (8.3%) and two-wheeler (11.1%) accidents were less common causes of craniofacial trauma. All patients who had self fall consumed alcohol and one patient sustained injury in a train accident (Figure-2). Pattern of injury Most common areas involved were upper face (36.1%) and lower face (25%) followed by combination of upper and middle face (11.1%). Other areas were less commonly involved (Figure-3) Clinical features and treatment Clinical features associated with different type of facial fractures are shown in table 1. Headache and vomiting were most common clinical features followed by loss of consciousness. Closed head injury was the most common neurological injury (14 cases) followed by skull fractures (5 cases).Most patients with upper facial fractures or combination of it had associated injuries (25 injuries) particularly closed head injuries and skull fractures (Table 2). One patient with upper facial injury had dorsal spine fracture with paraplegia. Ten patients were treated conservatively and 5 required neurosurgical intervention (2 for evacuation of subdural haematoma and 3 for compound depressed skull fracture). Minor procedures were performed in 8 patients including suturing of laceration and wound debridement. Eighteen patients had open reduction and internal fixation for facial bone fractures. There was no mortality. Discussion In the present study patients in 3rd and 4th decade were most frequently affected, an incidence similar to other reports identifying the relationship between facial fractures and concomitant neurologic injury. 6 - 8 However, the mean age (32.64 years) is higher in our study in comparison to others. 9, 10 There is male predilection for the combination of facial fractures and neurologic injury and the reported incidence varies from 47% to as high as 91%. 6, - 8 Young males were more affected (55.5%) with a peak in third decade in present study, which is consistent with other reports. 6 - 9, 11, 12 Table 1: Location of facial fractures and clinical features in 36 patients
Figures in parenthesis are
percentages Table 2: Distribution of facial fracture and associated injuries in 36 patients
Figures in parenthesis are
percentages Motor vehicular accidents were the most frequent cause of combined cranial and facial fractures followed by fall from height, particularly from coconut tree (our centre is situated in a coastal area). In other reports, motor vehicular accidents are also the major cause of cranial as well as facial injuries. 6 - 9, 14 - 18 Prevalence varies depending on the demographics and geography of the area and it may change with time. 11, 12 The anatomic composition of the upper and middle facial makes them more susceptible to fracture compared with the mandible. 15, 16, 19In the present report, upper facial skeleton was involved in 63.6% cases followed by lower face. Headache (88.8%) and vomiting (86.1%) were the most common clinical features in present study followed by loss of consciousness (75%) and all were more common in patients with fractures of upper and middle face. Patients with involvement of upper and middle face had more incidence of nasal bleeding. Oral bleeding was commonly associated with lower and middle facial fractures and ear bleed was associated with upper facial fractures. In this report, the incidence of loss of consciousness in fractures of upper face was 85.7%, middle face 100% and lower face 50%/. The reported incidence of loss of consciousness in relation to facial fractures is 10.8% - 55%. 6, 8, 20Historically, the facial architecture has been perceived to be a cushion against impact, protecting the neurocranium from severe injury. 9, 21 However recent investigations have suggested that the face (particularly upper and middle face) may actually transmit forces directly to the neurocranium, resulting in more serious neurological injuries. 6 - 9Injuries to upper and middle facial region significantly increase the risk of neurological injury and are crucial in the assessment of patients with craniofacial trauma. 2, 5, 8, 22 – 24 Lower facial injuries in the present report was associated with low incidence of loss of consciousness and other injuries. It has been hypothesized that when the mandible sustains fewer fractures, the dissipation of energy is reduced and more force is transmitted to the cranial vault, thereby resulting in a higher incidence of loss of consciousness. 25 Multiple fracture patterns likely serve as a neuroprotective mechanism, allowing greater dissipation of forces and resulting in less residual energy to be transmitted to the cranial vault. 25 Craniofacial injuries particularly of upper and middle face are associated with increased risk of neurological and other injuries and immediate neurosurgical intervention is frequently required. A timely detection and prompt treatment should lead to improve results and outcome.25 - 27 This report shows that injury patterns in developing countries, particularly in rural areas may not be different from developed countries, and control needs to follow similar preventive measures. References
Copyright 2006 - Annals of African Medicine The following images related to this document are available:Photo images[am06008t1.jpg] [am06008t2.jpg] [am06008f3.jpg] [am06008f2.jpg] [am06008f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}