 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 5, No. 1, 2006, pp. 46-51 Hypoglycaemia in Fasting Low Birth Weight Infants in Jos, Nigeria 1S. Pam, 2E. Ejeliogu, 3V. Pam, 2I. Madziga, J. Collins, B. Toma and 1O. Adekwu Departments of 1Paediatrics and 2Obstetrics and Gynaecology, JosUniversity Teaching Hospital, and 3Department of Human Physiology, University of Jos, Jos, Nigeria Reprint requests to: Dr. S. Pam, GPO Box 789, Jos, Nigeria. E-mail: sundaypam@yahoo.co.uk Code Number: am06011 Abstract Background/Objective: Low birth
weight (LBW) infants are commonly at risk of hypoglycaemia. The prevalence of
hypoglycaemia and its neurological features in fasting LBW infants below 24
hours of age was assessed. Key words: Hypoglycaemia, low birth weight, fasting, common, neurological manifestation Résumé Fond/Objectif: Les enfants de poid faible à la naissance (PFN) sont
généralement en danger de hypoglycémie. La prévalence de l’hypoglycémie et de
ses dispositifs neurologiques dans la sans-alimentation des enfants de PFN
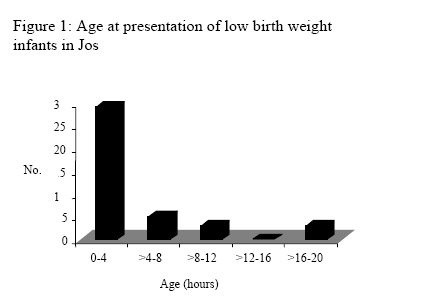
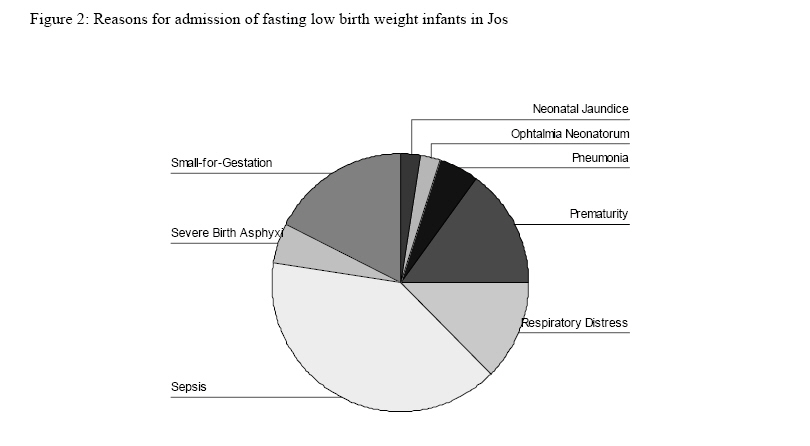
sous l’ âge de 24 heures a été évaluée. Mots clés: Hypoglycémie, poid faible à la naissance, sans-alimentation, terrain commun, manifestation neurologique Introduction The newborn’s brain relies on glucose for essential metabolism.1 The newborn is considered to be in a state of transition with respect to glucose metabolism, from complete dependence in utero, to complete independence.2 Consequently, hypoglycaemia is very common after birth. In normal newborn infants, blood sugar actually drops to a nadir in the first 1-3 hours. Higher levels are attained thereafter due to mobilization of glucose from glycogen and early feeds. Glycogen reserves are lower in low birth weight infants (LBW), as a result of shorter period of deposition and increased utilization in utero, especially in the small-for-gestational age infants (SGA).3 Besides, immediate postpartum hyperinsulinism suppresses gluconeogenesis and lipolysis, further increasing demand for glucose. A study in Nepal, 4 demonstrated that hypoglycaemia was more common in infants who were preterm, of lower birth weight, polycythaemic and those with smaller head size among others. Hypoglycaemia occurs in 50% of SGA infants, typically in the first 12 hours of life.5 In a study of 56 infants with hypoglycaemia, Cornblath et al observed the following symptoms: convulsions, apnoea, apathy, high-pitched cry, limpness, refusal to suck and eye-rolling.6 It has been observed by some that symptoms may be absent in hypoglycaemia, consequently, it is preferred to screen all infants at risk.7 LBW infants are commonly at risk of hypoglycaemia. At the Jos University Teaching Hospital, many LBW infants presenting to the newborn intensive care unit are not fed early by parents on account of the worry of what to do for such small and sick newborn. This study, therefore, aimed at describing just how common hypoglycaemia is and how frequently it manifests with neurological features in these high-risk LBW infants who have not had food or water in first 24 hours of life. Patients and Methods This prospective study was conducted at the Special Care Baby Unit of the Jos University Teaching Hospital, Jos Nigeria. It is a 500-bed tertiary Hospital in north central Nigeria, whose referral area spans 6 of Nigeria’s 36 states. It serves both as a secondary and a tertiary centre because of its peculiar location and costs being affordable to both the rich and poor. The newborn unit has a bed capacity of 30, but frequently stretched to 35 and has an annual patient turn-over of 702 infants. Commonest indications for admission are neonatal jaundice, sepsis and prematurity. The nurse to patient ratio varies from 1 to 7 during morning shift to 1 to 15 during night shift. It serves as a training centre in neonatology for resident doctors in Paediatrics, and Obstetrics and Gynaecology, medical students as well post-basic nurses in midwifery and intensive care. For the purpose of this study, the following definitions were used: hypoglycaemia was defined as blood sugar level below 2.2 mmol/l; Low birth weight infant (LBW) as an infant whose birth weight is <2500 grammes; Moderately Low birth weight infant (MLBW) as one whose birth weight is between 1500 to <2500 grammes; Very Low birth Weight (VLBW) as an infant with birth weight between 1000 and <1500 grammes; Extremely Low birth weight (ELBW) as an infant born with a weight >500 grammes but <1000 grammes. All consecutive LBW infants seen in the first 24 hours of life from September 2000 to April 2001 in the Special Care baby Unit (SCBU) of the Jos University Teaching Hospital, Jos, Nigeria were considered for recruitment. This period spanned the end of the rainy season through the cold dry season and early in the rainy season of the following year. Parental consent was sought for and obtained prior to inclusion in the study. History of prior feeds was sought. Only those who had had no form of food or glucose-containing intravenous fluids from birth were included. Information was obtained to assess the presence of any neurological features associated with hypoglycaemia in the infants as follows: tremors, convulsions, apnoea, and refusal to suck. The maturity of these infants was determined, based on Dubowitz method, to be preterm, preterm SGA or Term SGA. Age of mother, her parity and place of delivery were also recorded. The infant then had heel-prick blood sample taken for random blood sugar, using the Refloflux glucometer, a strip-based test. It measures blood sugar in the range from 0.5 to 27.7 mmol/l. Infants with blood sugar below 2.2 mmol/l were treated by giving 4 ml/kg of 10% dextrose solution intravenously followed by maintenance 100 ml/kg per 24 hours. All infants who could feed were given breast milk or formula as soon as this was feasible. Random blood sugar was assessed two hours after treatment to ensure that there was correction. No attempt was made to modify this practice during the period of the study. Other tests and treatment were given to infants as dictated by their clinical condition. Data was analysed using EPI Info version 3.2.2 and SPSS version 11.0. Results A total of 40 infants were eligible and all satisfied the inclusion criteria and so were recruited from September 12, 2000 to April 20, 2001. During the same period, there were a total of 155 LBW infants (79 Males: 76 Females) out of a total of 345 (M: F, 1:0.67) newborn infants seen in the unit, giving a fasting incidence of 25.81%. The LBW infants seen in the period were distributed as follows: ELBW 14 (9%), VLBW 40 (25.8%) and MLBW 101 (65.2%) Characteristics of infants The distribution of age at presentation was positively skewed (Figure 1), with median of 2.5 (range 0.33 to 19) hours. There were 27 males and 13 females with a gender (M: F) ratio of 1: 0.48. Mean birth weight of the infants was 1.413±0.319 (range 0.904 to 2.200) kg. When the birth weights were categorized, there were 6 (15%) ELBW, 13 (32.5%) VLBW and 21 (52.5%) MLBW infants. Majority 28 (70%) of the infants were preterm appropriate-for-gestational age infants, 10 (25%) were preterm small-for-gestational age and only 2 (5%) were term small-for-gestational age. All the infants came to the ward because they had one form of ailment or the other (Figure 2). Place of birth Majority 25 (62.5%) of our infants were born in our hospital, all of whom presented to our unit before the age of 6 hours, mean (±SD) age at presentation being 1.49(±1.10) (range 0.33 to 4) hours. Before attaining the age of 6 hours, 33 (82.5%) of all the infants, irrespective of place of birth, had presented to our unit. Blood sugar The proportion of infants with hypoglycaemia was 26/40 (65%). Infants with hypoglycaemia according to birth weight category were as follows: ELBW 3 (50%), VLBW 10 (76.9%) and MLBW 13 (61.9%). The corresponding number of hypoglycaemic infants based on maturity were found to be 19 (67.9%) preterm, 6 (60%) preterm SGA and 1 (50%) Term SGA. When the SGA infants were grouped together irrespective of whether Preterm or Term, the odds ratio (95%CI) for hypoglycaemia was 1.51 with 95% confidence interval of 0.37 to 6.08) (Table 1). This difference was not significant. Hypoglycaemia was not significantly different between infants born in our hospital compared to those born outside. When 2 arbitrary cut off-points for age at presentation (4 and 6 hours) were used, the incidence of hypoglycaemia was not found to be significantly different between infants (Table 2). Linear regression of infants’ blood sugar against mothers’ age gave a coefficient of 0.033 (p=0.403). Parity of mother, age of infant at presentation, and birth weight had no significant relationship with blood sugar either. All hypoglycaemic infants responded to correction of the blood sugar as described earlier. None of the infants demonstrated any neurological feature of hypoglycaemia throughout the period of the study. Packed cell volume Mean PCV was 51.2±8.5 (range 33 to 65) %. Only one (2.5%) infant had a PCV below 35%. There were 12 (30%) infants with PCV greater than 55%. Hypoglycaemia was not significantly different in infants with PCV greater than 55% compared to those with PCV ≤55% (Table 3). Table 1: Blood sugar levels according and maturity of low birth weight infants in Jos
p = 0.72 Table 2: Hypoglycaemia and time of presentation of low birth weight infants in Jos
Table 3: Blood sugar levels and packed cell volume low birth weight infants in Jos
p =0.562 Discussion The major finding in this report is that hypoglycaemia is indeed common in LBW infants who have not been fed in the first 24 hours of life. Our prevalence of hypoglycaemia at 65% is higher than 11% reported from Nepal.4 Our population of LBW infants was at risk for hypoglycaemia on account of sickness, LBW/prematurity and fasting. The infants from Nepal were those who were not admitted in the SCBU. We chose to look at fasting LBW infants in order to assess the seriousness of hypoglycaemia in this vulnerable group. There were few SGA infants relative to preterm appropriate-for-gestational age infants. Perhaps, if the reverse were true, the prevalence could have been higher, since hypoglycaemia is a recognized problem in SGA infants. It is noteworthy that our infants had absolutely no documented neurological feature of hypoglycaemia. The question might be asked as to whether they could be considered as truly hypoglycaemic. The definition of hypoglycaemia has been controversial for a very long time. Whipple’s triad would appear to be the definition of clinically significant hypoglycemia.8 However, this leaves out asymptomatic hypoglycaemia. Other approaches to defining hypoglycaemia include the epidemiologic based on cut-off point, acute effects on neurological functions and an approach based on neurological long-term outcome.2,8 Whether an infant manifests with hypoglycaemia seems to depend on the availability of other nutrients for use, commonly triggered by natural compensatory mechanism of lipolysis and gluconeogenesis. In a study of apparently healthy infants in Nepal, De Costello et al found that absence of antenatal care was associated with better counter regulation in response to low blood glucose levels.9 Their explanation was that these women, who failed to attend antenatal care, were those who were not well nourished and the attendant stress placed on the infants by the mothers’ poor nutritional status could have triggered the compensatory mechanisms earlier. This may largely be the case in our infants who were all fasting and admitted for one ailment or the other. It is crucial to reiterate at this point that prior to this study, seizures have not been commonly observed in our newborn infants with documented hypoglycaemia. Failure of the body to use alternative fuels such as fatty acids and ketone bodies, causes symptomatic hypoglycemia.1 This seems to give support to the role of alternative fuels in preventing clinical manifestation of hypoglycaemia. The clinical acumen of the clinicians involved in our study is not in doubt. While most of them were registrars of not less than 6 months experience in Paediatrics, some were house officers and all involved were detailed on the features to look for. Subtle neurological signs of disease in the LBW could be missed even in the hands of the expert, except careful and repeated examinations are done. Documentation of any repeat assessment of clinical features beyond the 2 hour post correction of hypoglycaemia was not done in this study. It could be argued as to why time of presentation did not significantly affect blood sugar levels. The results show that the proportion of infants with hypoglycaemia presenting late was higher than that those presenting early, irrespective of the time cut off point of 4 or 6 hours. Perhaps, a larger sample size is required to demonstrate a significant relationship. Hypoglycaemia was not affected by maturity of infant at birth nor was it affected by PCV difference when an arbitrary cut point of PCV>55% was used. While cut-off points for hypoglycaemia generally vary between experts, it is agreed that euglycemia should be in the range between 2.5 to 7.5 mmol/l.1,2 In our population, LBW SGA infants constituted less than a third of the total, and true term SGA infants were only 2 (2.5%). Besides, both preterm LBW and SGA are prone to hypoglycaemia. Consequently, for any statistically significant difference in blood sugar levels to be observed between the two groups, a larger sample size would be required. It needs to be restated that the primary aim of the study was not to show this difference, but to look at LBW as a single group. It is recommended that further studies should assess the difference in blood sugar levels between preterm and SGA LBW infants. Early feeding is expected to decrease the frequency of hypoglycaemia, particularly in these infants who are vulnerable. This message must be carried down to mothers more seriously. Though our hospital is recognized as a Baby Friendly facility with early breastfeeding actively encouraged, the need to feed small infants early certainly deserves a special emphasis. The Refloflux Glucometer is a very handy instrument in our setting where the use of the hexokinase assay method for blood sugar not only takes long but lack of regular quality control may invalidate the results. In Pakistan, it has been shown that the Glucometer is a good screening tool for infants with symptomatic hypoglycaemia.7 In a study in which 5 glucometers were compared, none was found to be completely reliable in demonstrating hypoglycaemia.10 We believe that glucometers have a place in screening for hypoglycaemia, especially, were the sole aim is to treat, to prevent the attendant consequences on the newborn infant’s brain. Our study aimed at screening for hypoglycaemia with the intention to treat. In all our infants, hypoglycaemia was corrected with standard protocol. Blood sugar levels are dynamic, being affected by so many neonatal factors, including feeding, disease, temperature changes and drug administration. Consequently, frequent monitoring of blood sugar is pertinent. This may be challenging especially in our setting where time to obtain results could be very long and besides anaemia requiring transfusion may result from blood loss due to repeated sampling.11 In situations of more serious causes of hypoglycaemia such as hyperinsulinameic hypoglycaemia, regular sugar monitoring is absolutely necessary.12 Infants requiring long-term glucose monitoring should benefit from long term subcutaneous micro dialysis which has been proven to have very high sensitivity, specificity, and positive and negative predictive values.13 It would be useful to define the blood sugar decay pattern in these fasting LBW infants. This could indeed reveal the possibility and extent of use of alternative fuels for metabolism in our population. Hypoglycaemia is a common problem in our LBW infants who have not been fed in first 24 hours. The role of alternative fuels in hypoglycaemic LBW infants in Jos needs further assessment by future studies. High index of suspicion is necessary to screen for hypoglycaemia. Early feeding of these infants needs to be stressed further. These should decrease the incidence of hypoglycaemia and attendant complications. Acknowledgment We are grateful to Professor John Ibu, formally of the Department of Human Physiology, University of Jos, Nigeria, who criticized the original protocol; Jane Njihia, Canada who criticised the complete manuscript and to the numerous staff of Special Care Baby Unit of Jos University Teaching Hospital, Jos, Nigeria. References
The following images related to this document are available:Photo images[am06011t1.jpg] [am06011f2.jpg] [am06011f1.jpg] [am06011t3.jpg] [am06011t2.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}