 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
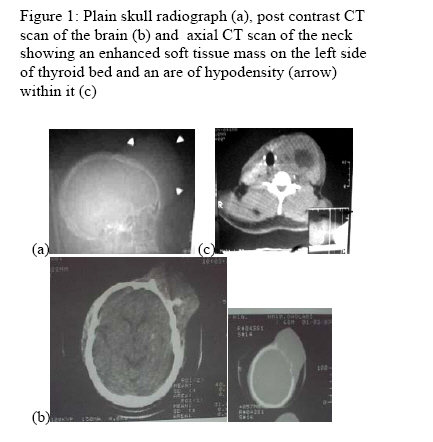
Annals of African Medicine, Vol. 5, No. 1, 2006, pp. 60-61 LETTERS TO THE EDITOR Follicular Thyroid Carcinoma Presenting With Skull Metastasis after 24 Years P. O. Ibinaiye, A. O. Adeyinka and M. O. Obajimi Department of Radiology, University College Hospital, Ibadan, Nigeria Dear Editor, Follicular thyroid carcinoma (FTC) originates in follicular cells and is the second most common cancer of the thyroid after the papillary carcinoma. 1The skeleton is one of the principal targets of metastasis from FTC. 1 FTC with distant metastasis is considered a relatively progressive tumour associated with a poor five-year survival rate. 1 A case of FTC presenting with skull metastases after 24years of initial diagnosis is presented. A 66-year-old male who had presented earlier in 1976 (twenty four years ago), at the surgical out patient clinic of the University College Hospital, Ibadan, with a small soft tissue anterior neck swelling which was asymptomatic. Fine needle aspiration of the mass done at that time confirmed follicular thyroid carcinoma. The patient declined the option of total thyroidectomy, and was discharge against medical advice and was lost to follow up He later represented in the year 2000, on account of a huge progressive and painless swelling on the skull and anterior neck. The examination revealed an anterior scalp mass which was attached to the skull and measured 18x16x10cm, soft to firm in consistency. The anterior neck mass moved with act of swallowing and measured 20x18cm, soft to firm in consistency. The thyroid function test showed elevated T3=233.6mIu/dl (normal: 100-190MIu/dl). The T4, TSH, Ca2+ and PO42- were normal. The skull radiograph (Figure 1) showed a soft tissue mass overlying the left frontal bone. . The Brain computed tomography (CT) scan (Figure 1) showed an enhancing soft tissue mass overlying the fronto-parietal bone with destruction of the underlying bone and some bone fragments were seen within it. There was no intracranial extension. Radiograph of soft tissue of the neck showed a huge soft tissue mass in the anterior neck, more on the left side. No calcification or lucency was seen within it. There was associated retro-sternal extension with displacement of the trachea posteriorly and to the right side. The axial CT scan (Figure 1) slices of the neck showed an enhanced soft tissue mass on the left side of the thyroid bed, with associated hypodensity within it. The outline was smooth and there was compression of the trachea and displacement of both trachea and larynx to the right side. No underlying bone destruction was seen. The lumbosacral spine radiograph showed metastatic destruction of the pedicle of L3 on the right, while the chest radiograph confirmed retrosternal extension of the neck mass. Fine needle aspirations of thyroid and the skull frontal masses confirmed follicular thyroid carcinoma and metastases respectively. Total thyroidectomy and left frontal craniectomy and tumor excision was done. The skull mass was seen to destroy the underlying bone with extension to the underlying dura matter. During the excision of the skull tumor, the patient developed uncontrolled bleeding and died of disseminated intravascular coagulopathy intraoperatively. FTC occurs more frequently in whites than in blacks and incidence is higher in women than men. FTC is common in all age groups, with a mean age of 49 years and an age range of 15-84 years. This case report is of the black race in a 66 years old male. Follicular thyroid carcinomas (FTC) comprise 10% to 20% of all thyroid carcinomas 2 and in areas of iodine deficiency this number may be increased. The thyroid gland is also particularly sensitive to the effects of ionizing radiation. Exposure to ionizing radiation results in a 30% risk for thyroid cancer and a history of head and neck X-ray taken especially during childhood, has been recognized as an important contributing factor for the development of thyroid cancer. Chest radiograph, CT scan and MRI usually are not used in initial workup of a thyroid nodule, except in patients with a clear metastatic disease at presentation, as demonstrated by the patient in this case report. These tests are second-level diagnostic tools and are useful in preoperative patient assessment. The soft tissue radiograph of the neck may show a soft tissue mass in the anterior neck displacing and compressing the trachea. There may be associated retrosternal extension with calcifications. This case report demonstrated all these features except calcifications. The typical appearances of a bony metastasis from thyroid carcinoma seen on plain radiograph could be an expansile, osteolytic lesion, which may be bubbly or have a blowout feature and often the lesion is solitary 2 as seen in this case. On ultrasonography, virtually all thyroid carcinomas are poorly echogenic with the majority showing some invasion into thyroid stroma and through the thyroid capsule on using high frequency probe in the ranged of 7.5 MHZ .2 A characteristic feature of these lesions is the presence of small calcifications or psammoma bodies on the ultrasound scan. 2 The thyroid gland is well seen on CT due to its higher than average soft tissue attenuation, caused by the physiologically high iodine content of the gland. Thyroid adenomas and carcinomas are seen as soft tissue masses within the gland. Calcification and cyst formation is seen in both types of lesion and CT cannot reliably distinguish benign from malignant thyroid masses unless metastatic disease, bone or cartilage destruction or neurological involvement is identified in the latter. 2 The retrosternal extension of thyroid mass can be demonstrated. Most of these features of CT scan were demonstrated in this case repot. Total thyroidectomy has become the routine procedure for treatment of FTC in Nigeria. 3 About 4-6 weeks after surgical thyroid removal patients must have radioiodine examination to detect and destroy any metastases and any residual tissue in the thyroid. Therapy is administered until radioiodine uptake is completely absent. 3 FTC prognosis is related to age, sex and staging of the disease. In general, if cancer is not extending beyond the capsule of the gland, life expectancy is minimally affected. Prognosis is better in female patients and in patients younger than 40 years. These findings were in sharp contrast to what was found in this report, in which the patient, a 66 year old male, lived with FTC without treatment for twenty four years after the initial diagnosis without symptoms. He only sought medical attention for cosmetic reasons on account of the neck and skull masses. The extensive search through available literature did not reveal report of similar case. References
Copyright 2006 - Annals of African Medicine The following images related to this document are available:Photo images[am06015f1.jpg] |
| |||||||||

{kind=link}