 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
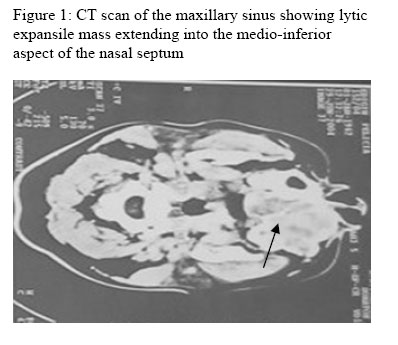
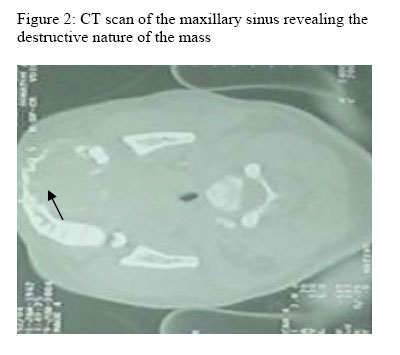
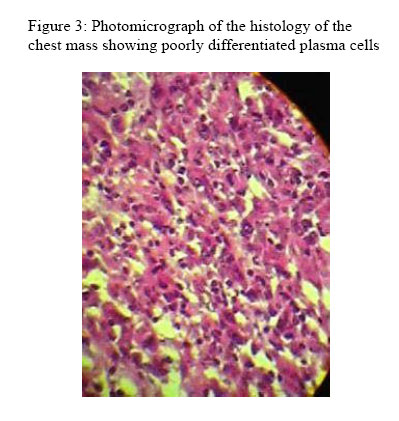
Annals of African Medicine, Vol. 5, No. 2, 2006, pp. 107-110 Two Rare Presentations of Plasma Cell Neoplasm C. E. Omoti Department of Haematology, University of Benin Teaching Hospital, Benin City, Nigeria Reprint requests to: Dr. C. E. Omoti, Department of Haematology, University of Benin Teaching Hospital, P. M. B. 1111, Benin City, Nigeria. E-mail: ediomoti@yahoo.com Code Number: am06025 AbstractA case of extramedullary plasmacytoma (EMP) in a 50year old woman and another case of solitary plasmacytoma of bone (SPB) with myeloma in a 34year old young man is reported. Atypical features of the SPB with myeloma patient were: a) age of the patient; b) lack of typical features of multiple myeloma (renal failure, hypercalcaemia and bone pain). The maxillary sinus was the site of the EMP who was referred for surgical excision. Biochemistry and haematological parameters were within normal range for both cases. Monoclonal paraprotein on serum electrophoresis was absent in EMP while it was present in SPB. Radiotherapy alone was given to the EMP patient while four courses of VAD (vincristine, adriamycine and dexamethasone) chemotherapy in addition to radiotherapy was given to the SPB with myeloma patient. Although EMP and SPB are both localized forms of plasma cell dyscrasias, SPB seems to have a greater tendency to multiple myeloma. Key words:Extramedullary, plasmacytoma, maxillary sinus, solitary, rib Résumé Il s’agit d’un cas du plasmacytome extramédullaire (PEM) chez une femme âgée du 50 ans et un autre cas du plasmacytome solitaire d’os (PSO) avec myélome chez un jeune homme âgé de 34 ans, Un trait typique du PSO chez un patient atteint du myélome étaient (a) âge du patient, (b) pénurie des traits typiques de myélome multiple (insuffisance rénale, hypercalcémie et douleur d’os). Le sinus maxillaire était le siège de PEM qui était envoyée pour une excision chirurgicale. Biochimie et paramètre hématologiques étaient dans des limites de la tranche normale des deux cas, paraprotéine sur le sérum électrophorèse était absent en PEM tandis qu’il est présent chez PSO. Le patient atteint du PEM avait eu la radiothérapie seulement tandis que quatre cours de VAD (vincristine adriamycine et dexamethasone) chimiothérapie en plus de la radiothérapie était donné au patient myélome avec PSO. Quoique PEM et PSO les deux sont des formes localisées de plasma cellule dyscasie. Il parait que le PSO a une tendance plus élevée pour myélome multiple. Mot cles :Extremédullaire, plasmacytome, sinus maxillaire, solitaire, côte Introduction Plasma cell neoplasms constitute a continuum of disease spectrum which have been classified as multiple myeloma (MM), solitary plasmacytoma (SP) and extramedullary plasmacytoma (EMP).1 SP is a rare localized form of clonal neoplastic plasma cell proliferation producing a solitary destructive bone lesion. Solitary EMP is an uncommon localized plasma cell malignancy mainly located in the upper aerodigestive tract or the head and neck region.2 These 3 entities cannot be differentiated from each other on a histological basis, and for this reason, clinical evaluation is important in their differential diagnosis. It has even been reported that EMP tends to be characterized by an indolent clinical course and lower incidence of progression to MM, and by definition they cannot occur within the bone.3, 4 At initial presentation of the localized myeloma, diagnosis is based on histological confirmation of monoclonal plasma cell infiltration of a single disease site and on the exclusion of systemic myeloma.5 However, the occurrence of a skeletal plasmacytoma which is truly solitary and thus curable is doubtless and certainly exceptional. In this paper two different cases involving SP of the rib and EMP of the maxillary sinus are reported, together with a review of the literature. Case 1A 50-year old woman presented with a progressive swelling in the region of her mouth of 25 months duration. The swelling was said to be painless, slow growing and causing no symptoms. She had excision biopsy at the dental clinic, which showed that the mass was a benign lesion. Patient however defaulted in clinic attendance for follow-up and over the years noticed a recurrence of the oral swelling which was non-progressive. Two years later, in June 2004 she presented in the ear nose and throat (ENT) clinic with a 1-month history of a progressive, painless growth in the left nasal cavity in addition to left facial swelling resulting from a protrusion in the oral cavity. There was no associated right nasal obstruction or recurrent catarrh and cough. No history of epistaxis or discharge of any kind from the affected nostril, no difficulty in swallowing or history of weight loss. Because of the partial occlusion of the nostril she resorted to occasional mouth breathing and native medication all to no avail. Physical examination revealed an obese woman with facial swelling over the left maxilla and lower eyelid. There was no lymph node enlargement. Physical and nasal endoscopic examination showed a deviated nasal septum, as well as a fleshy swelling that was sensitive, firm and no bleeding on contact. Examination of the throat revealed a palatal bulge into the oral cavity with an intact overlying mucosa, irregular swelling which does not bleed on contact. Conventional X-ray of the paranasal sinuses showed a soft tissue mass in the left maxillary sinus eroding the adjacent bones and encroaching into the left nasal turbinate. StagingCT scan of the affected area revealed an opaque maxillary sinus and lytic expansile mass extending into the medio-inferior aspect of the maxilla and bulging of the nasal septum into the ipsilateral nasal cavity (Figure 1). Also, the bone scan of the affected region revealed the destructive nature of the mass (Figure 2). A provisional diagnosis of a probable malignant left maxillary tumor was made. There was no morphological/quantitative abnormality of the haemopoietic lineages. Haematocrit was 0.43l/l, white cell count (WBC) 4.5x109/l with differential counts of neutrophils 54%, lymphocytes 44% and monocytes 2%, platelet count 300x109/l, and erythrocyte sedimentation rate (ESR) 24mm/1hour. Biochemical analysis revealed only increased glucose serum level (155mg/dl). A Caldwell-Luc operation was performed and biopsy of the soft tissue taken for histology. The histopatholgic diagnosis was compatible with extramedullary plasmacytoma (EMP). A comprehensive work-up including bone marrow aspiration and biopsy, total-body skeletal survey, determination of urine Bence Jones protein and serum monoclonal protein, chest radiograph and urinalysis were carried out to rule out MM. All of these studies were unremarkable in terms of systemic disease and therefore the patient was diagnosed as having a solitary EMP of the maxillary sinus. The patient was referred for radiation therapy, receiving 20rads per 10days and is on follow-up. Seven months post diagnosis, the patient continues to be in remission. She has no evidence of disease and the haematological and biochemical parameters are within normal range with the glucose serum level back to normal after diet therapy. Case 2 A 34year old young man presented in our institution on July 2004 with a 7month history of progressive swelling over the right anterior chest wall. There was minimal restriction of motion in the right arm. A positive history of anorexia, weakness/easy fatiguability and minimal weight loss 6 months before presentation was elicited. There was no similar swelling elsewhere in the body. There was no history of bone pain, fever; difficulty in swallowing, dyspnoea, palpitation, orthpnoea and his personal and family history was unremarkable. Physical examination revealed a right-sided anterior chest wall tumor extending from the fifth to sixth ribs. The mass measured 12x10cm, hemispherical with a smooth edge, slightly firm in consistency, nontender, not attached to skin but attached to underlying structures, not pulsatile and no bruit was heard. There was no associated lymph node enlargement. Haematological profile was: haemogram 15.5g/dl, WBC 7.8 x 109/l (differential count: neutrophils 60%, lymphocytes 40%), platelet count 333 x 109/l and ESR was 48mm/1hour. Biochemistry analysis was normal. Total skeletal survey showed no abnormalities but a chest-x-ray revealed osteolytic lesions in the anterior third of the right sixth rib with overlying soft tissue swelling, suggestive of a solitary plasmacytoma of the rib bone. A total surgical resection of the affected area was performed and the tissue sent for histology. The histopathologic diagnosis was compatible with solitary plasmacytoma of poorly differentiated plasma cells (Figure 3). Bone marrow cytology revealed a hypercellular marrow with evenly dispersed atypical plasma cells, also confirmed by the biopsy. Monoclonal peak was seen on serum protein electrophoresis and urinary Bence Jones protein was positive. Serum globulin was 3.1g/dl. The serum was negative for human immunodeficiency virus antibodies, and hepatitis C virus and hepatitis B surface antigens. Based on the clinical data, radiological, histological and electrophoretic findings, diagnosis of solitary plasmacytoma of the rib co-existing with multiple myeloma was made. Subsequently, the patient was commenced on VAD (vincristine, adriamycin and dexamethasone) chemotherapy after a course of radiotherapy. He was also placed on intravenous perfloxacine 200mg 12hrly for 10days. After the fourth course of VAD chemotherapy the patient had no limitation of motion in the affected right shoulder joint. However, patient has since left for better treatment option abroad for a possible bone marrow transplant considering his young age. Plasmacytomas exceptionally remain in a single skeletal segment and almost in all cases is followed by skeletal dissemination and poor outcome after several years.6 The SPB and EMP are unusual solitary tumors of plasma cell origin and their relationship to MM are still unclear, but they can be distinguished by their different clinical course. MM has histologic features identical to but clinically distinguishable from localized plasmacytoma. However, MM and SPB are similar histologically but clinically dissimilar to EMP.7 Multiple myeloma most commonly affects vertebral column followed by trunk and upper end of the femur, while in stage III disease most of the skeleton is usually affected.8 In each case, the rib and maxillary sinus which are rare were affected. Previous studies have reported better survival rates for EMP compared to SPB.5, 9, 10 Hence, SPB has further been classified as either latent or aggressive.11 The former is histologically well-differentiated while the latter is a poorly differentiated tumor which easily progresses to MM like the mentioned case of SPB co-existing with myeloma. The poor outcome may be due to the aggressive poorly differentiated form of the tumor. Hence, the reason for applying VAD chemotherapy in addition to the presence of serum and urinary paraprotein as earlier reported.11 In contradistinction, in the case of EMP of maxillary sinus only radiotherapy was given since there was absence of paraprotein in serum and urine. This supports the theory that SPB and EMP are distinct disease entities.12 It has even been reported that EMP co-exists with MM in only 5% of cases, but accounts for 3% of plasma cell tumor.10, 13 Treatment of plasma cell dyscrasias varies and depends on whether the disease is solitary or disseminated especially those that start in an indolent manner like the present case. Radiotherapy is still the treatment of choice for localized myeloma as given in the case of EMP while systemic chemotherapy is given to severe and poorly differentiated plasma cells at first contact. Also, the place of bone marrow transplant cannot be ruled out in order to prevent a local recurrence, as occurs in 6% of patients.14 References
Copyright 2006 - Annals of African Medicine The following images related to this document are available:Photo images[am06025f1.jpg] [am06025f3.jpg] [am06025f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}