 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
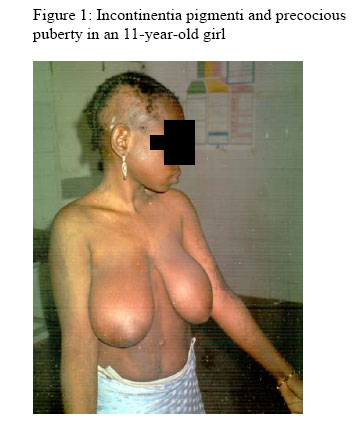
Annals of African Medicine, Vol. 5, No. 2, 2006, pp. 111-113 Pigmenti Associated With Precocious Puberty: Case Report 1R. D. Wammanda, 1H. W. Idris, 1S. Musa, 2N. D. Chom and 3S. A. Akuyam Departments of 1Paediatrics, 2Radiology and 3Chemical Pathology, AhmaduBelloUniversity Teaching Hospital, Zaria, Nigeria Reprint requests to: Dr. R. D Wammanda, Department of Paediatrics, AhmaduBelloUniversity Teaching Hospital, Zaria, Nigeria. E-mail : wammanda@yahoo.com Code Number: am06026 AbstractAn 11-year old girl, born at term following an uneventful pregnancy, had some blisters on both sides of the head and discrete but linear vesiculobullous lesions on the arms and the trunk at birth. Months later, she developed hyperpigmented lesions over the areas of the vesiculobullous lesions. She achieved menarche at the age of 7 years and by 9 years, had fully developed secondary sexual characteristics. Her bone age was advanced and had luteinizing hormone and follicular stimulating hormone in the pubertal range. Our patient has demonstrated a rare clinical association of incontinentia pigmenti with idiopathic precocious puberty. The clinical significance of this association of incontinentia pigmenti with precocious puberty is not known. Key words:Incontinentia pigmenti, precocious puberty Résumé Une fille âgée de 11 ans née pendant la période à la suite d’une grossesse sans incidents avait eu quelques ampoules dans les deux côtés de la tête et lésions vesiculobilaire (linéaire) discrète mais linéaire sur les bras et le tronc à la naissance. Quelques mois plus tard, elle a atteint des lésions hyperpigmentées dans les régions des lésions vesculobiliaires. Elle a atteint du menarche à l’âge de 7 ans et à l’âge de 9 ans elle avait parfaitement dévelopé des caractéristiques sexuels secondaires. L’âge de son os était avancé avec des homones luteinées et des hormones stimulantes folliculaire dans la zone pubertale. Notre patient avait démontré une association clinique rare d’incontinentia pigmenti avec la puberté précoce idiopathique. L’importance clinique de cette association d’incontinentia pigmenti avec précoce puberté n’est pas connu. Mot clés : Incontinentia pigmenti puberté précoce Introduction Incontinentia pigmenti is a rare multisystemic X-linked dominant disorder which is usually lethal in males.1, 2 Over 80% of cases of incontinentia pigmenti are caused by mutation affecting the NEMO gene resulting in defective activation of the transcription factor, nuclear factor-kappa B (NF-B), an essential partway in the antiapoptotic and proliferative cellular mechanism.2, 3The skin lesion usually manifests as four cutaneous stages: vesiculobullous, verrucous, linear hyperpigmented and atrophic lesions.2, 4 These cutaneous lesions in all stages tend to follow Blaschko lines, a system of lines on the surface of the body representing the typical pattern that the linear nevi follow. 5 All stages do not necessarily occur in a patient.2, 6, 7 The inflammatory and hyperpigmented stages are the most consistent of these cutaneous lesions.2 The course of incontinentia pigmenti is relatively benign, the irregular pigmentation usually fades leaving no traces in adulthood. 2, 8 Incontinentia pigmenti has been associated with ocular and dental anomalies as well as anomalies of the nails, hair, skeleton, central nervous system and cardiovascular anomalies.2, 4, 9 There has been no report of its association with sexual precocity. This case is therefore being reported as a rare clinical case of incontinentia pigmenti associated with precocious puberty in an 11 year old girl. Case reportAn 11-year-old girl presented with blisters on both sides of the head, which were noticed from birth. These blisters later progressed to form bullae that subsequently ruptured, discharging clear but slimy fluid. These lesions healed and left areas devoid of hair on both temporoparietal areas of the scalp. At about the same time, areas of discrete but linear vesiculobullous eruptions were noted on the arms, and the trunk. These lesions later coalesced and healed. About 2 months later, warty lesions appeared overlaying the previous areas of the vesiculobullous areas and months later, the progressive development of the present hyperpigmentations commenced. These skin lesions do not itch. There was no history of seizures, hearing impairment or visual disturbances. She achieved menarche at the age of 7 years and by 9 years had fully developed secondary sexual characteristics. Parents were not blood related and no other member of the family has similar skin changes or history of sexual precocity. Examination showed linear hyperpigmentations over the arms and the trunk (Figure 1) with bilateral scaring over the temporoparietal areas of the scalp. She had bilateral megamesia, fully developed axillary and pubic hairs. Her height was 162cm, > 95th centile for her age and sex. Examination did not show evidence of any focal neurological abnormality. Her serum urea and electrolytes, as well as the full blood counts and differentials were all normal. Abdominopelvic ultrasound showed a normal adult size uterus with the maximal anterio-posterior (AP) diameter being 22.7mm. The adnexia were normal. The pelvic X-ray showed the appearance of secondary epiphyses of both iliac crests (the adolescent sign). The secondary epiphyses of the head of femur, the lesser and greater tronchanters of the femur were almost fused. Her bone age was consistent with a patient between the ages of 16 and 18 years. The luteinizing and follicular stimulating hormones were 5.1mIU and 3.1mIU respectively, all within the pubertal range. Detailed neuroimaging studies with magnetic resonance imaging (MRI) or computerized tomography (CT) were not done due to lack of such facilities. Discussion Since the initial description of incontinentia pigmenti (Bloch-Sulzberger Syndrome) by Bloch and Sulzberger in 1926 and 1928 respectively, several other cases of incontinentia pigmenti have been reported in the world literature.9 This syndrome is characterized by frequent association with ocular and dental anomalies, as well as anomalies of the nails, hair, skeleton and central nervous system. Association of incontinentia pigment with phaeochromocytoma has also been reported. 8 Our patient demonstrates a rare clinical association of incontinentia pigmenti with precocious puberty. Although skin biopsy in patients with incontinentia pigmenti shows a type II cytotoxic inflammation (with macrophage phagocytosis of dyskeratotic keratinocytes and melanocytes), associated with eosinophilia, 2, 10 the diagnosis is made on clinical grounds. The diagnosis of incontinentia pigmenti in this patient was based on the description of vesiculobullous lesion at birth followed by hyperpigmented lession overlapping the previous area of the vesicobullous lesion. Although Blaschko linear hyperpigmentations can be observed in a heterogeneous group of mosaic conditions, such as hypomelanosis of Ito, these conditions are not associated with blistering phase in the neonatal period. 6, 11 Also the Naegeli syndrome, a rare entity similar to incontinentia pigmenti but without the blistering phase in the neonatal period and having abnormal enamel of the teeth, was ruled out because our patient did not present with the other features of this syndrome such as hypohidrosis and dystrophic nails. Apart from the vesicullation and the pigmented stages of incontinentia pigmenti, which may affect the scalp, patients with incontinentia pigmenti may have diffuse alopecia, some times accompanied by scarring. 12 Our patient has bilateral temporoparietal diffuse alopecia following the healing of the vesiculobullous lesions at birth. Whorled (spiral) pattern of alopecia that appears to correspond to the Blaschko’s lines in the scalp has also been reported 13. Scarring alopecia in incontinentia pigmenti is permanent and can be used as a marker to ascertain affected adult women who may no longer have the cutaneous manifestations. The patient was considered to have idiopathic precocious puberty because of the presence of obvious secondary sexual characteristics, advanced bone age, serum luteinizing and follicle stimulating hormone in the pubertal range and the absence of obvious central nervous system (CNS) tumour or other disorders of the CNS. However it is still possible that the patient’s precocious puberty could be due to a latent tumour such as a hypothalamic harmatoma, which can lie quiescent without causing features of space occupying lesion for many years. Studies have shown that clinical features, including the age of onset of puberty as well as endocrine investigations, are not good indicators of underlying pathology in girls with central precocious puberty.14, 15 McCune Albright syndrome, a clinical syndrome that consists of the triad of polyostotic fibrous dysplasia, cutaneous pigmentation and multiple endocrine abnormalities, 16 was ruled out in our patient because of the absence of fibrous dysplasia and cysts of the skull and long bones. Also in McCune Albright syndrome, the cutaneous lesions are café au lait macules, which are not the cutaneous lesions in our patient. What is not clear in this child is whether the Incontinentia Pigmenti and precocious puberty are coincidental, and therefore of little relevance to other clinicians encountering patients with one or both of these clinical problems or they are causally related. Could the ectodermal abnormalities that can occur in the skin and the central nervous system in incontinentia pigmenti affect the area of the hypothalamic pituitary axis and lead to precocious puberty? Therefore, whether the association of incontinentia pigmenti and precocious puberty is of prognostic significance will need further evaluation. It is hoped that this communication will alert physicians to the possible existence of this rare association of incontinentia pigmenti and precocious puberty. References
Copyright 2006 - Annals of African Medicine |

{kind=link}