 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 5, No. 3, 2006, pp. 138-141 A 10-Year Review of Failed Tracheal Intubation during Caesarean Section in Enugu, Nigeria Patrick U. Nze Department of Anaesthesia, University of Nigeria Teaching Hospital, Enugu, Nigeria Code Number: am06032 Abstract Background/Purpose:To study
the incidence and causes of failed tracheal intubation (FTI) during Caesarean
section in the University of Nigeria Teaching Hospital, Enugu over a 10-year
period. Key words:General anaesthesia, caesarean section, failed tracheal intubation Résumé Introduction/Objectif :Etudier la fréquence et des causes de l’insuccès de l’intubation
trachéale (IIT) pendant la césarienne au centre hospitalier universitaire
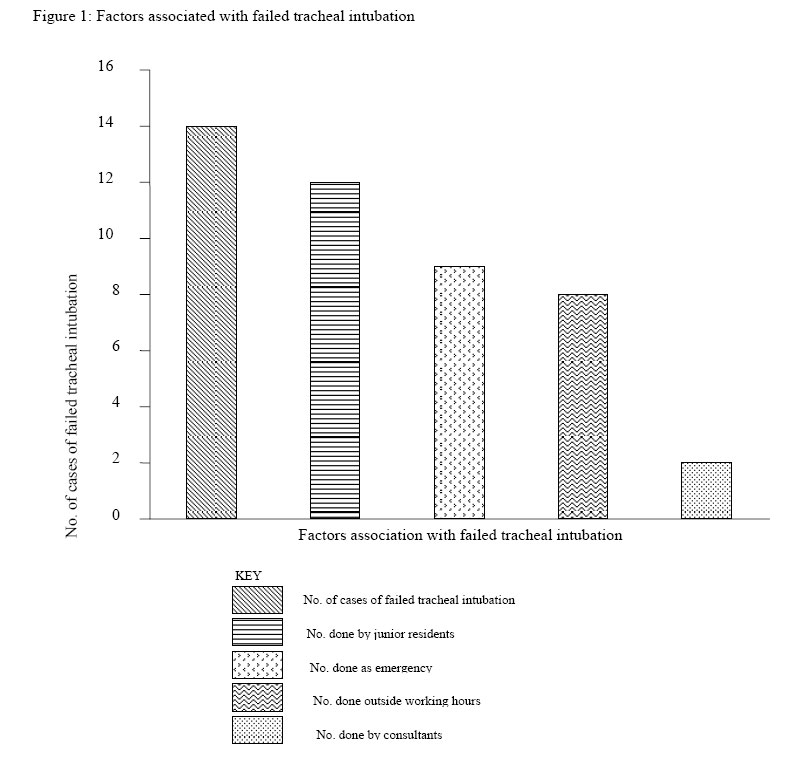
d’Enugu au cours d’une durée de 10 ans. Mot clés : Anesthésie générale, césarienne, intubation trachéale insuccès IntroductionEndotracheal intubation is required to provide a patent airway when patients are at risk for aspiration, when airway maintenance by mask is difficult and for prolonged controlled ventilation.1 Studies of difficult intubation suggest that there is a higher incidence of failed intubation in parturients (1:250).2, 3 During pregnancy changes occur to many systems. Of particular importance are those changes that affect the respiratory system (including the airway) and the gastrointestinal system.4 Difficult intubation, failed intubation, and misplacement of the tracheal tube in the oesophagus appear to account for the majority of maternal deaths associated with anaesthesia.5 Most of the deaths are due to hypoxia, secondary to difficult or failed intubation or to pulmonary aspiration of gastric contents.6 There have been a few reports from teaching hospitals detailing experiences of failed intubation in obstetric anaesthesia7-8 and of complications of general anaesthesia in obstetrics. The aim of this study is to evaluate the incidence and causes of FTI in Enugu from January 1993 to December 2002. Materials and Methods This is a retrospective study aimed at evaluating the incidence and causes of failed tracheal intubation during Caesarean section in a period of 10 years, from January 1993 to December 2002 at the University of Nigeria Teaching Hospital, Enugu. All the case records of women who underwent Caesarean section (C/S) during the study period were retrieved and analysed. These records were obtained from the labour ward register, obstetric theatre register, anaesthetic charts, and from medical records department. Data were collected on maternal age, booking status, time of operation, reason for operation, grade of anaesthetist, and anaesthetic technique employed when tracheal intubation failed. Failed intubation was defined as an intubation that was not accomplished with a single dose of suxamethonium. Results During the period under review (January 1993 to December 2002) there were 3710 cases of C/S under general anaesthesia. There were 14 cases of failed tracheal intubation, giving a 10-year incidence of 1/265 or 0.38%. The women concerned were of mean age 29.4 years (range 18 – 40 years) and mean weight 75.5 kg (range 60 – 97kg). Table 1 gives a more detailed description of each case. The cases are arranged temporally, case 1 having occurred first. Nine (64%) of the 14 cases occurred outside the normal working hours of 8am to 4pm. Most of the cases of C/S were due to pre-eclampsia (8/14 or 57%). Other reasons for C/S were previous C/S, obstructed labour, retained second twin and maternal request. Junior Residents (Registrars) were involved in 12 (85.7%) of the cases of FTI while consultant anaesthetists were involved in 2 (14.3%) (Figure 1). General anaesthesia after FTI was continued with facemask in 9 cases (Cases 1, 3, 4, 5, 6, 9, 10, 13, 14). Tracheal intubation became successful after a second dose of suxamethonium in 3 cases (cases 7, 8, 12). Spinal anaesthesia was employed on 2 occasions after FTI (cases 2 and 11). Table 1: Details of cases of failed tracheal intubation in University of Nigeria Teaching Hospital, Enugu, 1993 – 2002
The results of this survey give an overall 10-year incidence of failed tracheal intubation (FTI) of 1/265. This is not significantly different from previous reports which range variously between 1/250, 7 1/280, 1 1/3005 and 1/750.6 To the obstetric anaesthetist, none of the physiological changes of pregnancy is more significant than those pertaining to respiration. Most parturient present with markedly increased vascularity throughout the respiratory tract. This capillary engorgement can cause swelling of the mucosae of the nose, oropharynx, larynx and trachea. This problem may be further exacerbated by fluid overload or oedema associated with pre-eclampsia. In such cases, manipulation of the airway can result in profuse bleeding from the nose or oropharynx making endotracheal intubation difficult. Situations that lead to the administration of general anaesthesia are the need for emergency delivery of a foetus, contraindication to the use of regional anaesthesia, patient preference and unexpected prolonged or difficult surgery. All of these situations are stressful and because of the need to rapidly induce anaesthesia, alterations in technique may occur, making intubation more difficult. Added to this are inappropriately applied cricoid pressure and lack of expert assistance in the event that difficulty is encountered. A major problem identified in the confidential enquiry into maternal deaths from the United Kingdom is the inexperience of the individual doing the intubation, often without expert back-up. This is most likely to occur on nights and for emergencies. These findings are in line with the observations of Hawthorne et al.7 Relative easy of tracheal intubation reflects the experience and skill of the individual anaeathetist. However, from time to time every anaesthetist encounters a patient in whom tracheal intubation is either extremely difficult or impossible. There are two problems: firstly recognizing the potentially difficult intubation and planning how to overcome the problem, and secondly ensuring patient safety when planned intubation has failed. In the event of failure, there should be a previously prepared routine that can be followed without hesitation. Skilled help should always be available, and consultant assistance sought. All equipment required must be available immediately: 1) A second laryngoscope with sizes of blades; 2) A range of tracheal tubes of differing sizes; 3) Introducer; 4) Gum elastic bougies; 5) Minitracheostomy set; 6) Oesophageal obturator; 7) Magill forceps; 8) Range of oral airways; 9) Nasal airways. Tunstall first published a protocol for the management of FTI in obstetrics in 1976.9 Like more recent protocols, 10 the protocols in use in our hospital (UNTHE) were derived from tunstall’s original. A decision should be taken early that intubation is not possible; endless striving is dangerous. A failed intubation drill should be instituted immediately. The following measures are suggested: 1) Maintain cricoid pressure; 2) Place the patient head-down in the left lateral position; 3) Maintain oxygenation with 100% oxygen: manual ventilation of the lungs (with facemask) may be necessary until the effects of muscle relaxant have ceased; 4) Allow patient to waken, and summon help; 5) When senior help arrives, it may be appropriate to reinduce anaesthesia, and attempt to reintubate using additional equipment. Alternatively, regional anaesthesia may be employed. Our hospital protocol as stated above was followed closely in all the cases and there was no adverse maternal outcome. The confidential enquiries into Maternal Deaths have suggested that protocols be regularly rehearsed and practised. However, Cook and McCrirric11 found that while protocols were present in most hospitals they surveyed few hospitals practised them. The laryngeal mask airway (LMA) has found a place in the management of FTI12 and has been used C/S following FTI.13,14 If the operation must proceed after FTI it has been recommended that further muscle relaxant should not be given and that spontaneous ventilations be used.15,16 In the case of fetal distress or maternal haemorrhage, anaesthesia is probably better maintained using 40% oxygen in nitrous oxide and a volatile agent. Patient should be allowed to breathe spontaneously when the effects of suxamethonium have ceased. If regurgitation and/or aspiration occurs, a sample of the aspirate should be obtained for measurement of pH. When the operation is concluded, the patient should be treated symptomatically. Intermittent positive pressure ventilation should be instituted early if respiratory failure develops and the patient should be transferred to an intensive care unit. It is concluded from this study that the majority of cases of FTI are emergencies, occur out of normal working hours and involve anaesthetic trainees. It is suggested that thorough preoperative airway evaluation and adequate exposure of trainee anaesthetists to obstetric anaesthesia will help in reducing the incidence of failed tracheal intubation. References
Copyright 2006 - Annals of African Medicine The following images related to this document are available:Photo images[am06032t1.jpg] [am06032f1.jpg] |
| |||||||||

{kind=link}