 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 5, No. 4, 2006, pp. 197-203 Prevalence and Causes of Eye Diseases amongst Students in South-Western Nigeria 1A. I. Ajaiyeoba, 2M. A. Isawumi, 2A. O. Adeoye and 1T. S. Oluleye 1Department of Ophthalmology, University College
Hospital, Ibadan, and 2Ophthalmology Unit, Obafemi Awolowo
University Teaching Hospital, Ile-Ife, Nigeria Code Number: am06047 Abstract Background/Purpose: To assess the prevalence and identify the causes of
eye diseases among students in Ilesa east local government area, in
south-western Nigeria, so that prevention strategies could be mapped out. Key words: Vernal conjunctivitis, refractive error, squint, corneal opacity Résumé Introduction/Objectif : Evaluer la fréquence et identifier les causes
des maladies de l’oeil parmi des étudiants dans la zone gouvernmentale locale,
l’Est d’Ilesa, dans le sud-ouest du Nigéria, pour pouvoir élaborer des
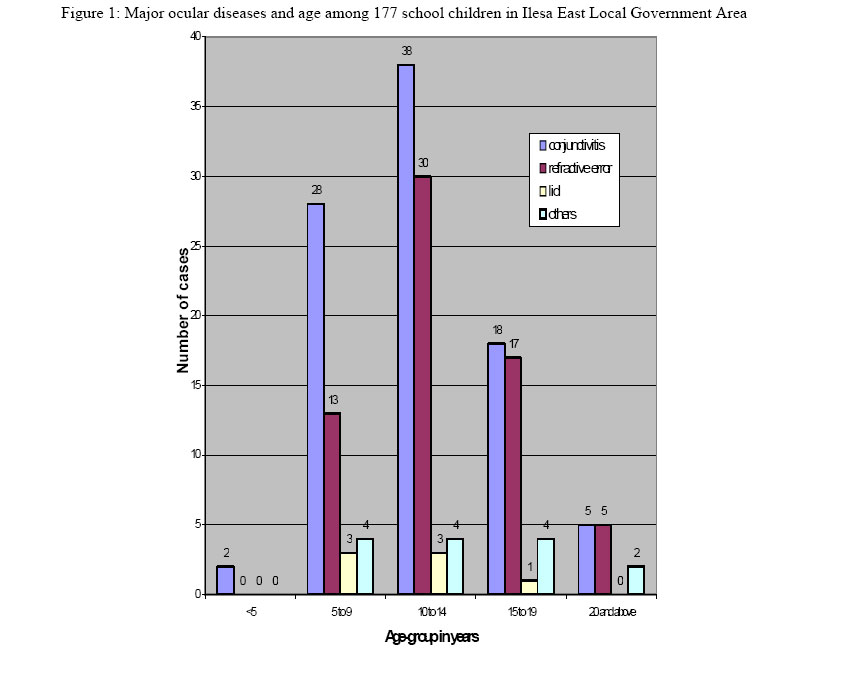
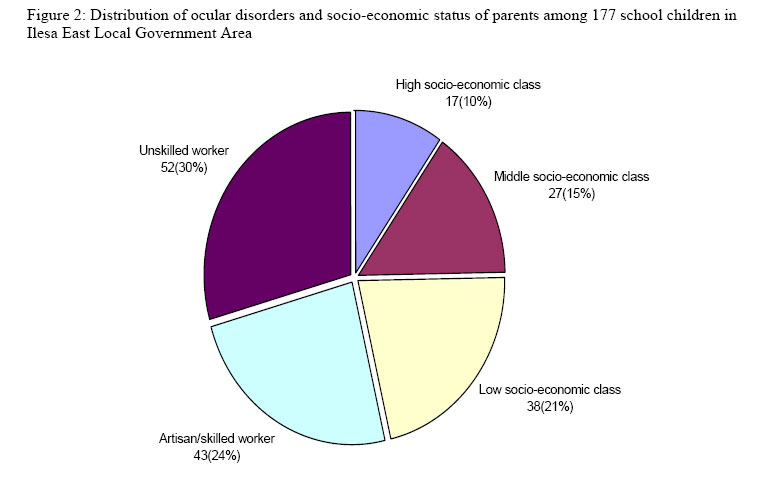
stratégies de prévention. Mots-clés: Conjunctivite vernale, erreurs de réfraction, yeux louches obscurité de la cornée Introduction The 5-19 years age group constitutes about 37.78% of the total population of Nigeria. 1 This age group is important since it forms the growing population whose potential dictates the country’s future economy. A study of the pattern of ocular diseases in children and young adults is very important because while some eye conditions are just causes of ocular morbidity, others invariably lead to blindness. Also while some conditions like refractive errors and cataract are treatable, others like trachoma and vitamin A deficiency are largely preventable. 2 Many studies on eye diseases in children carried out in the United Kingdom, Canada, and United States (USA) showed that the common ocular disorders in these countries were congenital or hereditary. 2 In Nigeria, hospital-based and school surveyson the pattern of eye diseases carried out in the south-western and eastern parts of the countryhave indicated that refractive errors, conjunctivitis, corneal scarring and injuries were some of the most common eye conditions affecting Nigerian children. 3, 4 This study was therefore designed to supply information about the pattern of ocular diseases in primary and secondary school students in Ilesa East Local Government Area in south-western Nigeria. Information obtained from the study will assist government in planning and facilitate the incorporation of primary eye care into the existing primary health care structure of the state. Materials and Methods A cross-sectional survey to assess the prevalence and identify the causes of eye diseases among students in Ilesa East local government area, in south-western Nigeria, was conducted during the months of February and April 2002. With a total population of primary and secondary school students being 28,703, and an average prevalence of 19.2% from previous studies; 5 - 7 the minimum sample size was calculated to be 745 using the universal formula. A 2-stage random sampling technique was then used to select 1144 students from 6 primary and 3 secondary schools (selected using the Epi-table) in Ilesa East Local Government Area. The first stage was selection of primary and secondary schools from the local government list of all schools in their area of jurisdiction. The second stage was the selection of students from the already selected primary and secondary schools. All the selected children participated in the study. Approval for the study was obtained from the Research and Ethical Committee of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria. Informed consent from the parents of students was obtained with the assistance of school heads through their class teachers. Teachers were trained and tested by the authors to obtain demographic data and perform visual acuity testing on the students. A pilot study was carried out in one primary and one secondary school not selected for the study. Every pupil or student selected at the 2nd stage random sampling was registered for the study. Their demographic data were obtained and recorded by the trained teachers. Information obtained included name, date of examination, and name of school, age, sex, class and father’s occupation. Snellen’s literate and an illiterate ‘E’ chart placed at 6 meters in a well-illuminated area were used to test the visual acuity (VA). VA was tested in all the students registered for the study by the trained teachers and ophthalmic nurses; separately for each eye and recorded according to World Health Organisation’s (WHO) classification. Near vision was assessed in both eyes using the ‘Sussex Vision Test Type. Any student that failed to read the 6/6 line had VA cross-checked by one of the authors (IMA) as well as checking with pin-hole. Students whose VA improved with pin-hole had refraction done by the optometrist at the base hospital. Ocular examination of the students was performed by one of the authors (IMA) using a pen torch and an ophthalmoscope in a darkened room. Those who needed immediate treatment for conditions like infective and mild to moderate vernal conjunctivitis were given prescriptions. Students who did not improve with pinhole were also invited to the base hospital for more detailed assessment and investigations such as dilated direct and indirect ophthalmoscopy using 0.5% mydriacyl drops and slit-lamp examination. Students with discharging/red eyes, severe vernal conjunctivitis, cataract, and blindness from any condition were given referral notes treatment, for follow up and counselling in the hospital. Parents of students with blindness and visual impairment were invited for interview where necessary in order to accurately determine the aetiology. A pre-designed data collection form was used to record information obtained. Specially designed computer software Epi Data 2.0 was used to enter data, carry out checks and rechecks to ensure validity. Data was analysed using computer software Epi lnfo version 6. Analysis included frequency distribution for the variables of interest and stratification by age groups, sex, schools and father’s occupation. P-values for test of significance were determined. Results A total of 1144 students were examined. These comprised 617 (54%) in 6 primary schools and 527(46%) in 3 secondary schools. Of these 504 (44.1%) were males while 640 (55%) were females. Their ages ranged between 4 and 24 years. The mean age was 11.89 years ± 3.52 SD. The 10-14 years and the 5-9 years age groups were the largest groups of students examined. Ocular diseases were observed in a total of 177 (15.5%) students. This comprised 75 primary school pupils with a prevalence of ocular disorders of 12.2% and 102 secondary school students with a prevalence of 19.3%. The major ocular disorders encountered in were conjunctival disorders, refractive error, lid disorders and corneal opacity (Table 1).Conjunctival diseases were the most prevalent ocular disorder occurring in 91 students (8%). Allergic/vernal conjunctivitis was seen in 85 students accounting for 7.4% of all the ocular diseases; especially the palpebral type (4.6%), followed by the limbal type (1.9%) and then the mixed type (0.9%). There were 2 cases each (0.2%) of non-trachomatous infective conjunctivitis and pseudopterygium. There were 2 unknown cases (0.2%) of abnormal appearance of the conjunctivae. Refractive error was the second common ocular disorder seen in 66 (5.8%) students. It was almost twice more common in females with 58 cases than in males with 33 cases. Only 2 children were wearing glasses, out of 4 previously diagnosed cases. There were 3 cases each of stye (0.3%) and ptosis (0.3%). Among those with ptosis, one had congenital bilateral ptosis while the other two were as a result of complications of vernal conjunctivitis. There was only 1 (0.1%) child with chalazion.Three children had corneal opacity giving a prevalence of (0.3%) of all cases. There was 1 case each of anterior staphyloma and bilateral keratoconus complicated with corneal opacities. There were 2 (0.2%) students with cataract. One had bilateral immature cataract associated with visual impairment while the other had an almost mature cataract associated with severe visual impairment. There was only 1 (0.1%) case of iritis. Three children had squint (0.3%). One had 450 esotropia secondary to traumatic corneal opacity and two exotropia at 300 and 450 associated with refractive error. Details of prevalence and distribution of ocular diseases amongst 117 students are summarised in Table 1. The prevalence of ocular diseases was highest (48%) among the 10-14 years age group, followed by the 15-19 years age group with (33.3%) (Figure 1). There was a significant female preponderance 67.2% in the distribution of ocular disorders, with a female: male ratio of 2:1(p <0.05). The father’s occupational status, which is an index of socio-economic status, showed an inverse relationship to the occurrence of ocular diseases amongst the students. Figure 2 illustrates a significant decreasing prevalence of ocular diseases as one climbs up the socio-economic ladder (p <0.05). Only 62 (35%) of the students with ocular diseases actually complained of eye symptoms whilst 115 (65%) did not complain of any ocular symptoms but diagnosed of ocular conditions (Table 2). Majority 1103(96.4%) had normal vision, 15(1.3%) had visual impairment while 2(0.1%) were bilaterally blind (Table 3). Table 1: Prevalence of ocular disorders among 177 school children in Ilesa East Local Government Area
Table 2: Prevalence and distribution of eye symptoms in 62 school children in Ilesa East Local Government Area
Table 3: Distribution of visual acuity among 1144 school children in Ilesa East Local Government Area
Discussion The overall prevalence of ocular morbidity among students in this study is similar to that found in Ibadan5 and Benin, 6 which are in the same geographical region. The prevalence of ocular diseases in our study is however lower compared to that found in Lagos7 also in the same geographical zone. This may be due to the large population found there, and the heterogeneous nature of the highly urbanised population. Our figure is also higher than that found in Enugu, 8 which could be attributable to ethnic differences. In the USA, a prevalence of significant causes of ocular conditions among school children was foundto be 28.8% and previously undetected ocular conditions being 19.8%.9 That prevalence almost doubles that in this study. Racial factors could be attributable Our experience in the pattern of ocular disorders seen in this study is similar to a study carried out in Anambra State where conjunctivitis, refractive errors, and lid disorders were most commonly found.10 Comparatively, the pattern as seen in Jos among school children showed that refractive error, chronic conjunctivitis and corneal scars were the commonest causes, with lid disorders ranking low. 11 Majority of the students in this study were below 18 years of age, this may explain why ocular disorders were mostly found among first, the 10-14 years age group followed by the 15-19 year age group and then the 5-9 year age group. This could be related to the occurrence of vernal conjunctivitis, which is common in children and young adults, reducing with advancing age as more persons in the 10 – 14 years age groups had more ocular pathology than those in the 5-9 years age group. Similarly, a reduction in the number of cases of vernal conjunctivitis above the age of 10 years was found in a study among post primary school students in northern Nigeria. 4Ocular disorders were found to be significantly commoner among the females. This could be due to the female preponderance in this study. Only a few of the students examined complained of eye problems while others were not even aware that they had eye problems. This experience is similar to that of other workers in different parts of the world in which 15% of children aged 3-5 years and 25% of children aged 6-17 years had vision problems which they were not aware of. 12 Among those children who complained, symptoms were mostly allergic in nature and those referable to asthenopia. This has strongly indicated the need to establish an early and continuous system of examining school children so as to prevent the occurrence of ocular morbidity. There was also an association between the occurrence of ocular disorders and the lower socio-economic class, which had higher prevalence of ocular disorders (p <0.05). Other studies have also confirmed this relationship. 7, 13 Apart from this, ignorance, lack of parental interest and poverty were the most likely contributory factors because there are eye units in both the General and Teaching Hospitals, all located within the town and easily accessed by all. This was further buttressed by the fact that despite free consultations for examination, most of the parents refused to bring their children for follow up treatment. Most encouraging however, was the fact that these common ocular disorders were not very expensive to manage. Although not usually a cause of blindness, vernal conjunctivitis has been found to be a leading cause of absenteeism from school. 3, 4 A hospital-based study found that vernal conjunctivitis was responsible for 25.3% of the cases seen. 3 The palpebral form was seen to be twice more common than the limbal form in this study as also observed by other workers. 14 Comparatively, studies done amongst primary school children in Tanzania showed that the prevalence of vernal conjunctivitis was very low (0.4%) while trachoma/infective conjunctivitis had a high prevalence of 5.6%. 15 The high prevalence of vernal conjunctivitis in this study could be due to the fact that the work was carried out during the rainy season. This has been attributed to high concentration of allergens indoors because of closed doors and windows by some authors.15 This study showed a female preponderance in all the disorders. This differs from a lot of other studiesthat have found male preponderance in the occurrence of vernal conjunctivitis.14, 15 This female preponderance may be due to the fact that more of them were seen in the study. However, it could also be related to application of cosmetics among the female students, which could then precipitate allergic conditions. The prevalence of refractive error obtained in this study falls within the WHO’srange of 2-10% worldwide. 16 The Tanzanian study had only (1.0%) prevalence and so could not justify a school eye screening programme in that locality solely for refractive error.13 There were many newly diagnosed refractive errors as was also the experience of some authors. 7 However only 2 children previously diagnosed were wearing corrective glasses. Poor vision and inability to read clearly materials written on the board can have a serious impact on the child’s participation and learning in class. This can therefore adversely affect the child’s education, occupation and socio-economic status for life. 16 Poor economic status of parents had been identified as a main constraint and barrier preventing children from wearing glasses. 17 This therefore calls for a lot of effort and work to be done by professionals about public health education towards the use of spectacle correction among students. Corneal diseases were the major causes of blindness and visual impairment. These were from keratoconus and bilateral corneal opacities that complicated vernal ulcers. This has strongly linked corneal diseases as the highest causes of blindness. 18 It has been suggested that heredity and environmental factors may contribute to the aetiology of keratoconus and corneal hydrops in Congolese children. 19 It was however surprising that corneal opacity post measles keratitis was not found in this study. It could have however co-existed with some other type of infective keratitis like bacterial. However, a change in the trend is being noticed, especially in areas of increased level of awareness, immunization, availability of ophthalmologist, eye hospital, and higher social standards. For example, a study carried out in a blind school in Lagos, showed that retinal dystrophy, followed by lens disorders constituted the major anatomical causes. 20 Unilateral causes of blindness were corneal opacity following trauma and cataract. 20 In our study, there was a case of unilateral blindness from post traumatic corneal opacity. Works done by many authors, show that school children and students of post primary institutions were particularly vulnerable to trauma with subsequent visual impairment or blindness especially while at play. 21, 22 Visual outcome depends on the type and extent of injuries. 22 The need for adult supervision of children at play, 3 and putting in place prevention or control measures, cannot be over emphasised. This study has similarly shown low rate of squint occurrence as previous workers in Nigeria. 6,7 Compared to studies done in developed countries, which usually have higher rates as seen in the Belfast study, where children born with very low birth weight followed up were found to develop squint. 23 It may be interesting to find out the relationship of our low birth weight babies who survive and the manifestation of squint in another study. External eye conditions such as stye, ptosis, and chalazion were not threat to vision. They however occurred more frequently in this study, ranking as the third common ocular disorders. However, other reports found these diseases ranking lowest. 4, 24 Only one case of iritis seemed to support uveitis being common in the young. Other workers with similar experience however found more of posterior, than anterior uveitis in our environment compared to the Caucasianpopulation.25, 26 Perhaps more studies need to be done to ascertain the recent trends in occurrence of this uncommon disease in children. In conclusion, ocular diseases are rampant amongst students in Nigeria. Prevention, early recognition and prompt treatment of these diseases by regular screening of students would definitely reduce ocular morbidity so that they can attain their full potential in the course of their education. Focus should be targeted on yearly school eye screening so as to identify treatable eye diseases and improve their knowledge of common eye diseases and their prevention; and correction of refractive errors. This will go a long way in the prevention of unnecessary blindness and visual impairment in the young. The socio-economic benefits of this cannot be over-emphasised. Information obtained from the study will assist government in planning; and facilitate the incorporation of primary eye care into the existing primary health care structure of the state. AcknowledgementWe are grateful to the local government inspector of education, principals, head-teachers, staff and students of the schools involved in this study. We are also grateful to Mr. Lasisi and Mr. Ajala for their assistance during the examination. References
Copyright 2006 - Annals of African Medicine The following images related to this document are available:Photo images[am06047f2.jpg] [am06047f1.jpg] |
| |||||||||

{kind=link}
{kind=link}