 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
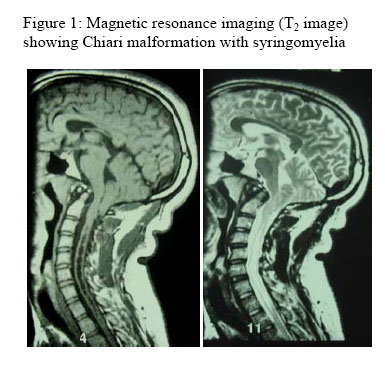
Annals of African Medicine, Vol. 5, No. 4, 2006, pp. 206-208 Chiari I Malformation: A Missed Diagnosis B. B. Shehu, N. J. Ismail, M. R. Mahmud and I. Hassan Division of Neurosurgery, Department of Surgery, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria Code Number: am06049 Abstract Chiari I malformation is a complex congenital malformation of the hindbrain, characterized by herniation of the cerebellar tonsils through the foramen magnum into the cervical spinal canal. There may be mild caudal displacement and flattening or kinking of the medulla with an associated small posterior fossa. We present a case of a 30 year old man who presented with a 2 year history of worsening nystagmus and ataxia with associated occipital headache and diplopia. Examination showed a young man with horizontal and vertical nystagmus, he had truncal ataxia and Rhomberg’s sign was positive. Diagnosis was missed by several clinicians during the 2 year period. Repeated brain CT scans were normal. Brain MRI confirmed the diagnosis of Chiari I malformation and cervical syringomyelia. He had decompressive occipital craniectomy durotomy and duroplasty. The patient recovered fully from ataxia headache and diplopia but still has residual nystagmus. Key words: Chiari I malformation, syringomyelia, posterior fossa, craniectomy, missed diagnosis Resumé La malformation Chiari I est une malformation congenitale complexe du cerveau posterior, characterisée par l’hernie de l’amygdale du cervelet dans le trou occipital et le canal spinal cervical. Il peut y’avoir le deplacement caudal, applatissement ou tortillement de la moelle allongée associé ã une petite fosse posterieur. Nous presentons un adult de 30 ans qui s’est presenté avec un nystagme progressive, l’ataxie associés à des. cephallées occipitales et la diplopie pour deux ans. L’examen de ce jeune homme revèle du nystagme horizontale et verticale, l’ataxie troncale avec le signe de Rhomberg present. Le diagnostique etait manqué durant ces deux années par plusieurs cliniciens. Des scanner repetés du cerveau etaient normaux. Le M.R.I. du cerveau a confirmé le diagnostique de la malformation Chiari I, ainsi que la syringomyelie cervicale. Il a eu une craniotomy decompressive occipitale (fosse cerebelleuse) durotomy ainsi que duroplastie. Le patient a eu une convallescence parfaite avec l’abolition de l’ataxie, les cephallées et la diplopie mais a encore du nystagme residuel. Mots clés: Malformation Chiari I, craniotomie de la fosse, cerebelleuse, diagnostique manqué Introduction Chiari malformation is one of the numerous abnormalities that may exist at the craniovertebral junction. It represents downward displacement of portions of the cerebellum, fourth ventricle and pons in varying degrees. It may be associated with syringomyelia. It is usually difficult to make accurate diagnosis from clinical features alone, especially in older patients and therefore, there is high rate of misdiagnosis. Earlier reported cases were from observations made on cadaveric specimens. The advent of magnetic resonance imaging (MRI) has made diagnosis of Chiari malformation and syringomyelia more reliable; however, cost and availability limits its use. Case report A 30-year old man presented with a 2 year history of worsening nystagmus and gait abnormality. Nystagmus was worst on straight gaze; there was diplopia, no ocular pain or visual impairment. The patient had persistent suboccipital headache and dizziness. There was no respiratory difficulty or cough. No history of trauma to the head, no seizures or loss of consciousness. He never had otitis media or tinnitus and no bowel or bladder dysfunction. His childhood development was normal and his performance in school average. He is a tailor, not a known diabetic or hypertensive. He does not drink alcohol or smoke cigarette; he is married and has two children. The patient had visited several hospitals in the past and all investigations done including repeated skull X-rays and brain computed tomogram (CT) did not give a clue to the diagnosis. He was then referred for Neurosurgical evaluation when the symptoms persisted. Examination showed a young man who was not pale, afebrile, and well built. The vital signs were all normal. The Glasgow coma score was 15; he had vertical and horizontal nystagmus, the pupils were equal and reactive to light. All cranial nerves were normal; the Rhomberg’s sign was positive and there was truncal ataxia, with the patient tilting towards the left. He had normal muscle power and tone in all limbs; deep tendon reflexes were exaggerated in all limbs, no ankle clonus, and Babinski’s response was flexor. Sensation of pain, touch, temperature, and joint position were normal. There was no sign of occult spinal dysraphysm. Examination of other systems did not reveal any abnormality. Packed cell volume was 38%, electrolytes, urea and blood sugars were all normal. ECG showed sinus tachycardia. Skull and cervical X-rays and brain CT scan did not show any abnormality. Cervical MRI showed inferiorly displaced cerebellar tonsil to level of C2 vertebra, downward displacement of the pons and medulla, beaked tectum, medullary kink, medullary spur a concave clivus and cervical syringomyelia (Figure 1). The overall features were those of Chiari I malformation with syringomyelia. The patient was prepared for surgery and he had decompressive occipital craniectomy, C1 + half C2 laminectomy, durotomy and dural patch graft. The findings at surgery were an adhesive band at the atlanto-occipital joint and dura with subdural gliosis and tonsillar herniation to C2 level. The syrinx was also noted and decompressed. Post operatively ceftriaxone, dexamethasone and ranitidine were given and was nursed 30° head up. The patient improved steadily, got relief from the suboccipital headache, diplopia and truncal ataxia, but still has residual nystagmus. Discussion Chiari malformation also referred to as hindbrain herniation or cerebellar ectopia was first described by Cleland in 1883, Chiari in 1891 and 1896 and Arnold 1894.1 - 3 It is the downward displacement of portions of the cerebellum, fourth ventricle, and pons, ranging in degree from: type I which is the caudal displacement of the cerebellum with peg-like tonsillar herniation below the foramen magnum, the medulla may be caudally displaced but the brainstem is not involved. Type II is characterized by downward displacement of the vermis, fourth ventricle, and lower brainstem into the spinal canal. Most cases occur in infancy and there is associated myelomeningocele and hydrocephalus. In type III there is displacement of nearly the entire cerebellum as well as the fourth ventricle into the cervical canal. Type IV is characterized by cerebellar hypoplasia without cerebellar herniation. Chiari malformation may be associated with other craniovertebral malformations and cranial nerve dysfunction. Hydromyelia and syringomyelia is present in 25% of patients with Chiari I malformation; the cervical cord is the most common site. Most patients have a small posterior cranial fossa. It is thought that Chiari I malformation may be a mesodermal disorder. Underdevelopment of the occipital somites of the paraxial mesoderm produces a small, overcrowded posterior cranial fossa. A small posterior cranial fossa underlies the development of acquired Chiari malformation in patients with craniosynostosis, hypophosphatemic rickets, achondroplasia, Paget’s disease and acromegaly.3 Acquired cases may also follow lumbar cerebrospinal fluid (CSF) shunting or ventriculoperitoneal shunt placement.2, 3, 6 The exact genetic defect is not known but it is known to be associated with other genetic diseases like achondroplasia, Klippel-Feil syndrome and Hadju-Cheney syndrome. There is a high rate of misdiagnosis in Chiari I malformation, mainly due to similarity of features with other central nervous system (CNS) diseases; even CT scan or MRI are known to miss the diagnosis. Hoh reviewed 364 cases and reported that 60% of the patients were misdiagnosed as having fibromyalgia, 31% misdiagnosed as migraine, 12% chronic fatigue syndrome and 9% multiple sclerosis. 63% of the patients were misdiagnosed as psychiatric malingering (most of the patients had multiple diagnosis) 5. Not surprisingly our patient was also misdiagnosed despite repeated clinic visits and investigations including brain CT scans. The age range of presentation of Chiari I malformation is 12- 73 years and average duration of presentation is 3.1 years. 6 The commonest symptom is suboccipital headache which is often brought about by neck extension, cough, Valsalva maneuver, or trauma. Other features include photophobia, diplopia, dizziness, nystagmus, ataxia, sensory or motor nerve deficits, cranial nerve palsies, palpitations, apnoea and spinal cord dysfunction which may be present in 94% of patients with syringomyelia. 3 MRI is the imaging modality of choice, as exemplified in our patient; bony and soft tissue abnormalities are easily visualized. CT has difficulty evaluating the foramen magnum region due to bony artifact; findings include tonsillar descent and ventricular dilatation. Skull and cervical spine X-rays may show bony abnormalities. Surgery is beneficial for symptomatic patients when done within 2 years of onset of symptoms. 6 Asymptomatic patients may be followed and operated upon if and when they become symptomatic. Patients who have been symptomatic and stable for years may be considered for observation, with surgery indicated for signs of deterioration. 6 The commonly performed surgery is posterior fossa decompression (suboccipital craniectomy), with or without dural patch grafting and cervical laminectomy of C1 through C2 or C3. The outcome of surgery is good especially when it is done early enough; some symptoms may not respond especially motor weakness and sensory deficit. Surgery also arrests the progression of the disease. 6 Chiari malformation is not uncommon, and the features may mimic other disease conditions; thus, accounting for the high rate of misdiagnosis. A high index of suspicion is required to make a diagnosis. Cervical MRI still remains the imaging modality of choice, and early suboccipital craniectomy may cure the symptoms. References
Copyright 2006 - Annals of African Medicine The following images related to this document are available:Photo images[am06049f1.jpg] |
| |||||||||

{kind=link}