 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
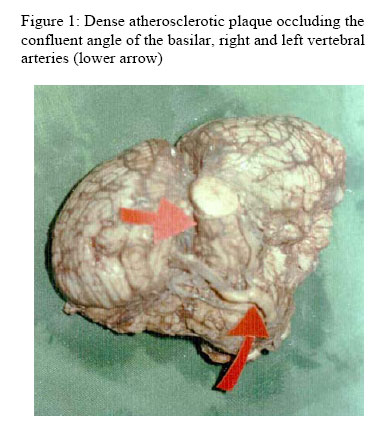
Annals of African Medicine, Vol. 5, No. 4, 2006, pp. 212-213 Apparently Asymptomatic Atherosclerosis of the Vertebrobasilar Arteries A. Mohammed and S. J. Maisamari Department of Pathology, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria Code Number: am06051 The brain specimen (Figure 1) was from an apparently healthy 50-year-old man, who died one hour after sudden collapse. The was no history suggestive of systemic hypertension or diabetes, except for complaints of chest pain of undetermined origin. On external autopsy examination he appeared well nourished, with no external injuries. Internal examination showed 0.3 - 0.5cm calcification and atheromatous changes in areas of all branches of the coronary arteries, restricted to the walls. There was 90% thrombotic occlusion of the first 5cm of the anterior left descending branch of the left coronary artery. There were four healed subendocardial fibrous scars (1 - 1.5cm) involving the apical myocardium. There were extensive atheromatous changes involving the basilar artery, near total occlusion of the vertebral arteries and aneurysmal rupture. Many branches of the circulus arteriosus were affected. The anterior, middle and posterior cerebral arteries show moderate congestion only. 100mls of subarachnoid hemorrhage was recovered from the posterior fossa. Little factual information concerning the frequency of different types of vascular brain diseases is available in the literature from this part of the world, where autopsies are relatively uncommon. This becomes more significant regarding fatalities due to cerebrovascular accidents. There was no history suggestive of transient ischemic attacks in this case, which should be expected over significant period. The survival of this patient prior to his death most probably was due to the dynamic cerebral system of circulation having within itself multiple reservoirs of possible collateral circulation.1 The involvement of several vessels may suggest a common type of atherosclerotic intracranial aneurysms that affect older adults usually arising in the setting of advanced and generalized cerebrovascular atheromatosis. This may assume many variant2, 3 which are saccular, fusiform, cylindrical and conical. Fusiform lesions of the vertebrobasilar trunk are the single most common variant.4the vertebrobasilar lesions in our case was the fusiform variant. Another possibility, especially due to involvement of the circle of Willis and basilar arteries is atherosclerotic ‘dolichoectasia’ (diffuse dilatation and tortuous elongation of the basilar or internal carotid arteries) and the two processes may coexist.4 This pathology can be acquired from atherosclerosis or as a congenital type with additional deficiencies in the muscular media layer.5the congenital type is also less likely to result to significant subarachnoid hemorrhage. 6 - 8 Atherosclerotic dolichoectasia is the more common type and is seen predominantly in the proximal vertebrobasilar arteries followed by internal carotid arteries. The age of onset is usually greater than 40 years with a male predominance.9our case fits more to artherosclerotic dolichoectasia than congenital type. Hence the suspicion of concurrent development of cerebrovascular atherosclerosis with coronary artery atherosclerotic changes and other vessels too, should be foremost in the minds of the clinicians. In such cases the associated risk of rupture is usually underestimated and compression of neighboring structures by aneurysmal dilatation is most likely.3 Diagnostic options such as magnetic resonance imaging, cerebral angiography and duplex ultrasound are used in combination to have full picture of the pathology. Regarding our case, similar cases have done well in other parts of the world from prompt diagnosis and posterior fossa decompression following such episodes.10 We believe our case is that of apparently asymptomatic atherosclerotic dolichoectasia of the vertebrobasilar arteries, with the involvement of circle of Willis and the coronary arteries. References
Copyright 2006 - Annals of African Medicine The following images related to this document are available:Photo images[am06051f1.jpg] |
| |||||||||

{kind=link}