 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
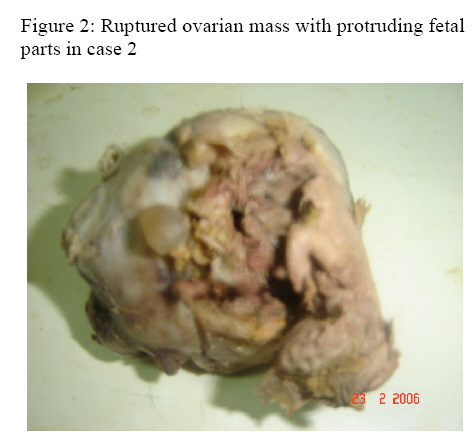
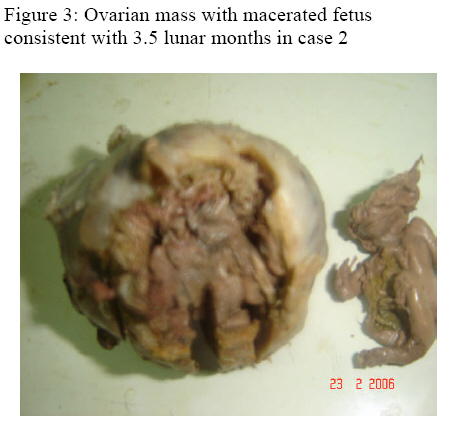
Annals of African Medicine, Vol. 6, No. 1, 2007, pp. 36-38 Ovarian Pregnancy Presenting as Ovarian Tumour: Report of 2 Cases 1M. O. A. Samaila, 2A. G. Adesiyun and 3L. M. D. Yusufu Departments of 1Pathology, 2Obstetrics and Gynaecology, and 3Surgery, Ahmadu Bello University Teaching Hospital, Shika –Zaria, Nigeria Reprint requests to: Dr M. O. A. Samaila, Department of Pathology, Ahmadu Bello University Teaching Hospital, Shika-Zaria, Nigeria. E-mail: mamak97@yahoo.com Code Number: am07009 Abstract We present 2 cases of ovarian masses diagnosed as tumours but turned out to be pregnancy. Ovarian pregnancy, a form of ectopic gestation has a distinct pathology though it can be a source of diagnostic difficulty clinically and intraoperatively. A total of 71 ectopic pregnancies were seen in the department from January 2001 to December 2005, of these only two were ovarian ectopics. Both patients were nulliparous and presented with lower abdominal pains, abdominal masses and menstrual irregularity. They both had laparotomy and total right salpingo-oophorectomy. Grossly, the ovaries were enlarged, grey tan and globular. Focal ruptures in the wall of the ovaries showed protruding fetal parts. Microscopy showed chorionic villi within and in continuity with ovarian stroma and corpus luteum. They were both diagnosed ovarian ectopics. A good knowledge and understanding of the gross pathology, combination of imaging studies and high index of suspicion should help in making an intra-operative diagnosis. Key word: Ovary, pregnancy, tumour Résume Nous présentons deux cas de masse ovariennes diagnostiques cliniquement comme des tumeurs mais après histologiquement ce sont révèles être des grossesses ectopiques. Les grossesses ovariennes, une forme de grossesse ectopique as une pathologie distincte est es difficilement diagnostiquée cliniquement. Un total de 71 grossesses ectopiques a été vues au Département de Pathologie entre Janvier 2001 et Décembre 2005. Deux grossesses étaient des grossesses ovariennes. Les deux patientes étaient nullipares et ce sont présentées avec des douleurs au bas ventre, des tumeurs abdominales et des menstruations irrégulières. Les deux ont eu une exploration abdominale suivie d’une salpingo-ovarectomie. Anatomiquement, les ovaires étaient, gris, globulaire, et hypertrophier. Des ruptures de la paroi ovaire montrait des protrusions d’éléments fœtal. Histologiquement les ovaires ont révélés les villosités chorioniques dans et en continuité avec le stroma ovarien et le corpus luteum. Les deux ovaires ont étaient diagnostiqués comme grossesse ovarienne. Une bonne connaissance et un bon entendement de l’anatomie-pathologie, une combinaison de l’imagerie et un fort taux de suspicion aide a faire un diagnostique clinique. Mots clés : Grossesse, ovarienne, tumeur Introduction Ovarian pregnancy, a form of ectopic gestation with a distinct pathology, can be a source of diagnostic difficulty clinically and intraoperatively.1 It shares similarity of presenting symptoms with other forms of extrauterine or ectopic pregnancy and ovarian tumours.4, 5 A total of 71 ectopic pregnancies and 173 cases of ovarian lesions were seen in the Department of Pathology, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria, from January 2001 to December 2005. Of these only two were ovarian ectopic pregnancies. This is a report of 2 ovarian pregnancies, mistaken clinically for tumours. Case reports Case 1: A 32year old nulliparous woman presented with a 4months history of lower abdominal pains and 6months history of irregular menstruation. Ultrasounography revealed right ovarian pregnancy which was removed at laparotomy. She had a right salpingo-oophorectomy. Grossly, a globular mass measuring 12x9cm and weighing 190g was seen. Parts of a well formed foetal skull and upper limbs protruded through a rupture in the mass. Part of tubal fimbria attached to the mass was also seen. Cut sections of the mass showed areas of haemorrhage and cystic dilations. Histology showed chorionic villi of varying sizes within ovarian stroma, extensive haemorrhage and corpus luteum (Figure 1). Case 2: A 27year old nulliparous woman presented with a six months history of right lower abdominal pains and regular menstruation. Investigations revealed a right ovarian mass which was considered a teratoma. At laparotomy, the mass which was still suspected to be a tumour was excised along with the right fallopian tube. Grossly, the ovary was enlarged and grey tan in appearance. It measured 8.5x6.5cm and weighed 120g. A small cyst and part of the fallopian tube fimbria was adherent to the ovarian wall. Cut sections showed grey and dark areas and a well formed foetus with macerated head and a crown rump length of 70mm consistent with three and half lunar months gestation (Figures 2 and 3). Histology showed chorionic villi within and in continuity with ovarian stroma, areas of haemorrhage and corpus luteum. Figure 1: Histology in case 1 showing chorionic villi (H & E x100) Figure 2: Ruptured ovarian mass with protruding fetal parts in case 2 Figure 3: Ovarian mass with macerated fetus consistent with 3.5 lunar months in case 2 Discussion Ovarian pregnancy results from the fertilization of a trapped ovum within the follicle or corpus luteum at the time of rupture.4, 6 Implantation within the ovarian stroma is aided by secretions of the corpus luteum. The fertilized ovum undergoes development with formation of placental tissue, amniotic sac and fetus.6 However, normal implantation occurs within the uterine cavity. The incidence of ectopic gestation is 4.5/1000 - 16.8/1000 pregnancies.4,7 Tubal pregnancy with an incidence rate of 1/200 - 1/300 pregnancies is the commonest form. 4, 8 The incidence of ovarian pregnancy ranges from 1/6000 - 1/40,000 pregnancies.9, 10 Ovarian pregnancy constitute 0.5% to 6% of all ectopic pregnancy, 1: 3000 of live births leading to a mean ovarian pregnancy per year of 1.6.9, 11-13 It comprised 1.2% of all ovarian lesions and 2.2% of all ectopic pregnancy in the present report, which compares favourably with other reports.9, 11-13 Ovarian pregnancy may present a clinical and operative diagnostic difficulty. 1-3 There are no specific clinical, laboratory or ultrasonographic signs to differentiate it from a tubal pregnancy.9 However, diagnosis should be based on a combination of rise in serum β-human chorionic gonadotrophin (hCG), ultrasonography and laparoscopy.3,14 The macroscopic characteristics of ovarian pregnancy should be helpful in making a laparoscopic or intra-operative diagnosis. These features include an intact fallopian tube and fimbria ovarica clearly separated from the ovary, a gestational sac located within the ovary and connected to the uterus by the ovarian ligament as well as demonstrable ovarian tissue in the sac.4 Histology remains the only means of confirming diagnosis of ovarian pregnancy with the presence of chorionic villi within and in continuity with ovarian stroma or a corpus luteum.4, 9, 11 A good knowledge of the gross pathology, along with imaging and high index of suspicion should help in making an intra-operative diagnosis of ovarian pregnancy. References
Copyright 2007 - Annals of African Medicine The following images related to this document are available:Photo images[am07009f2.jpg] [am07009f3.jpg] [am07009f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}