 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 6, No. 2, 2007, pp. 80-83 Dermatofibrosarcoma Protuberance: Case Reports 1M. E. Asuquo, 1M. S. Umoh and 2G. Ebughe Departments of 1Surgery and 2Pathology, University of Calabar Teaching Hospital, Calabar, Nigeria Reprint requests to: Dr. M. E. Asuquo, P. O. Box 1891 (GPO), Calabar, Nigeria. E-mail: mauefas@yahoo.com Code Number: am07020 Abstract Background: Dermatofibrosarcoma
protuberance (DFSP) is a relatively uncommon soft tissue neoplasm with
intermediate to low grade malignancy, rarely metastasizing to regional lymph
node or distant site but with proclivity for local recurrence due to inadequate
resection. Key words: Dermatofibrosarcoma protuberance, recurrence Résumé Introduction: Protubérance dermatofibrosarcome (DFSP) neoplasme
parties charnues rélativement peu commun avec une moyenne au niveau de la
malignité base, rarement métastazing à la lymphe ou siège à distance mais avec
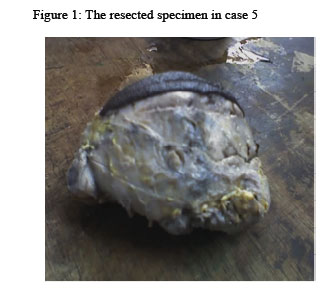
le penchant pour une récidive locale attribuable à la resection inadéquate. Mots-clés: Protubérance dermatofibrosarcome, récurrence Introduction Dermatofibrosarcoma protuberance (DFSP) is a relatively uncommon soft tissue neoplasm with intermediate to low grade malignancy.1, 2 It is a slow growing, locally aggressive fibrous tumour with a pronounced tendency to local recurrence, rarely metastasizing to regional lymph node or distant sites.3, 4 The relatively infrequent occurrence of DFSP lessens their clinical awareness and diagnosis is often made at histology.5 Most lesions occur over the trunk or proximal extremities.1 Recognition of this tumour is important because of the excellent prognosis after adequate surgical excision.5 We evaluated in this case reports the clinical histories of five consecutive patients obtained from histology request forms who had histologic diagnosis of DFSP in an attempt to identify the clinical characteristics of this tumour as a guide for adequate treatment and improved outcome. Case reports Case 1: A 26-year-old female presented with a history of a recurrent fungating mass in the right groin for one year. She had a previous surgery 8years ago in a private hospital facility and was not told what the lesion was. Later she noticed a recurrence, which began as a small swelling at the site of the previous excision. This progressively increased in size over 6months and later ulcerated with foul smelling discharge. Prior to this, she sought treatment in a traditional medical facility for which she had multiple incisions and topical herbal treatment to no avail. Examination revealed a patient in general good health with a fungating irregular nodular mass measuring 8 x 3.5 x 3cm. Excision biopsy revealed DFSP with the deep resection margins free of tumour. Postoperative period was uneventful. She was informed of the risk of recurrence and the need for follow up but defaulted after 3months. Case 2: A 35-year-old man presented with a recurrent chest wall tumour at a private hospital facility, details of previous treatment was not stated. There, he had an excision biopsy with skin grafting. Macroscopic features of the specimen were irregular greyish white tissue measuring 2.5 x 2 x 1.5cm. Cut surface showed a fish flesh appearance and histology revealed DFSP. Case 3: A 34-year-old man presented with a multilobulated recurrent mass in the right thigh of 9months duration with no regional lymphadenopathy. He had a previous operation 4years ago which was then thought to be a Lipoma in a private hospital. Later, he noticed a small mass at the site of the previous operation, which had progressively increased in size over the period of nine months and more after it was incised by a traditional medical practitioner who also applied topical herbal preparations. He later sought for treatment in another private hospital where he had an excision biopsy. An irregularly shaped greyish white tumour measuring 5 x 3 x 3cm sent for histology in this hospital revealed DFSP. Case 4: A 17-year-old woman presented with a painless multilobulated progressive right sided neck (supraclavicular) mass of 3 years duration, in a private hospital where she had an excision biopsy. There was no regional lymphadenopathy. A well-circumscribed fleshy mass measuring 8 x 5 x 5cm submitted for histology revealed DFSP with deep resection margin free of tumour. Case 5: A 20-year-old woman presented with a neck mass located in the right supraclavicular area of 10 months duration with no ipsilateral regional lymphadenopathy. She had an excision biopsy in a private hospital facility. A mass covered with elliptical skin measuring13cm across its widest diameter submitted for histology revealed DFSP with tumour extending to the deep resection margin (Figures 1 and 2)
Table 1: Summary of the 5 cases
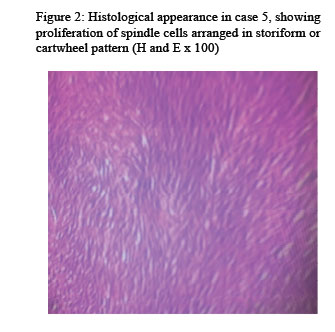
Discussion Dermatofibrosarcoma protuberance is an uncommon neoplasm in this population, five cases were seen between 2000 and 2004, a similar experience was reported by Ani et al.10 In the United States, it constitutes less than 0.1% of malignant neoplasms and approximately 1% of all soft tissue sarcoma.2 However, discrepancies in the reported frequency may be due to different terminologies and inconsistent histological pattern of the lesion.10 Hoffman in 1925 named this tumour as dermatofibrosarcoma protuberance,6 since then it has been described as hypertrophic morphea, progressive and recurrent dermatofibroma, fibrosarcoma of the skin and sarcomatous tumour resembling keloid. 3.5.7 Enzinger and Weiss developed a classification of soft tissue sarcoma using similarity of histological appearance to normal tissues, 8 however, the most widely used is that of the World Health Organization that classifies fibrous histiocytoma as a benign tumour, DFSP as intermediate tumour of fibrohistiocytic origin.9 Several studies reveal an almost equal sex distribution or a slight male preponderance.2 This report showed a female preponderance, (M: F of 2:3), with an age range of 17-35 years (mean 26.6 years, Table 1). These ages were apparently high as 3of the patients had recurrent lesions indicating they were younger at first presentation. This is in keeping with another study where the maximum incidence was in the 2nd and 3rd decades.2 This tumour has been reported in newborns, children and elderly individuals.2, 5, 11 The lesions involved the neck (supraclavicular) area in 2, trunk 2 and a case involving the proximal thigh. This is in keeping with other studies, 1, 5 where most reported lesions occurred over the trunk and proximal extremities. Mbome et al3 reported the lower limb and not the trunk as the site of predilection, Skoll et al12 reported acral dermatofibrosarcoma and Cione et al 12 a rare case involving the paediatric foot. Clinical presentation was that of painless, cutaneous, multilobulated mass in 3, in addition ulceration and pain occurred in the recurrent lesions 2. There was no regional lymphadenopathy, this is in keeping with other studies.10,14,15 In none of the cases was a histologic diagnosis obtained prior to excision which may have accounted for the limited resection with tumour at the margins in some cases. This tumour is not difficult to recognize because of its characteristic clinical appearance though some unusual variants have been reported.14 Clinicians are urged to be more aware of this condition10 and obtain a histologic diagnosis by core or incision biopsy prior to excision. Condensation of connective tissue at the periphery may give a false appearance of encapsulation but actually, tumour, may extend well beyond margins in microscopic projection.16 Recurrences are due to inadequate excision as reported in Case 5 with tumour extending to deep resection margin. Metastasis though rare may occur after repeated recurrences, 17, 18 as the lesion may become less well differentiated.19 Characteristic findings especially in nodular lesions are cellularlity and irregular, short, intersecting bands of tumour cells forming a storiform pattern or also cells radiating from a central hub of fibrous tissue forming a cartwheel pattern. Occasionally focal fibrosarcomatous changes with characteristic herringbone pattern may occur. The pigmented variant (melanin containing dendricites) known as Bednar tumour is another variant of this lesion. Immunohistochemistry using CD34 is a useful marker for the differentiation of DFSP from dermatofibroma. Immunostaining using CD34 is also helpful in identifying tumour cell at the surgical margins especially when treating recurrent DFSP where tumour cells are often interspersed within the scar tissue. Late presentation with large size tumours, (Figure 1) including recurrent lesions as depicted in this study militates against adequate excision, as the size may constitute a surgical challenge. Surgery is the main stay of treatment, wide excision with a safety margin of 3cm. including the underlying fascia is recommended, emphasis is on histology free margins for local control.4, 20 Computerized tomogram is helpful in deciding the line of incision and avoiding inadequate excision, which leads to recurrence or metastasis.21, 22 Mohs micrographic surgery has the advantage of high oncologic effectiveness and maximal tissue savingand is increasingly accepted as the treatment of choice.15 Chemotherapy is not used in the treatment of DFSP. Radiation hitherto with a limited role recently has been used as adjunct to surgery. The indications are in the positive resection margins, where wide excision also may result in major cosmetic or functional deficits. Molecular targeted therapy holds a promise for the future; Imatinib may provide an alternative treatment for unresectable tumours or adjunctive treatment in addition to surgery.2 Further outpatient care is important as the tumour has a proclivity for recurrence. Poor prognosis is characterized by its late presentation, aggressive local invasion, regional nodal involvement and distant metastasis. Some histologic features serve as poor prognostic indicators; high number of mitotic figures, increased cellularity, DNA aneuploidy, TP53 gene over expression and fibrosarcomatous change.2 In conclusion, DFSP is a rare tumour. Painless, cutaneous, and multilobulated lesions should arouse the suspicion of this tumour. These cases illustrate the need for histologic examination of all tissues removed at surgery. Core or incision biopsy should aim at pre-operative histologic diagnosis, adequate excision should be ensured to avoid recurrence for improved outcome and a decrease in the health care cost of this tumour. References
Copyright 2007 - Annals of African Medicine The following images related to this document are available:Photo images[am07020f1.jpg] [am07020f2.jpg] |
| |||||||||

{kind=link}
{kind=link}