 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 6, No. 4, 2007, pp. 190 – 193 Adult Laryngeal Rhabdomyosarcoma: Report of a Case and Literature Review A.Shayah1, F. O.Agada1, L.Karsai2 and N.Stafford1 1Department of Otolaryngology and Head and Neck
Surgery, Hull Royal Infirmary, Hull HU3 2JZ, United
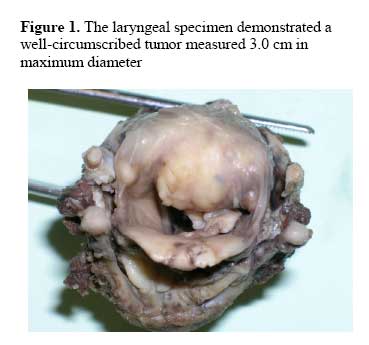
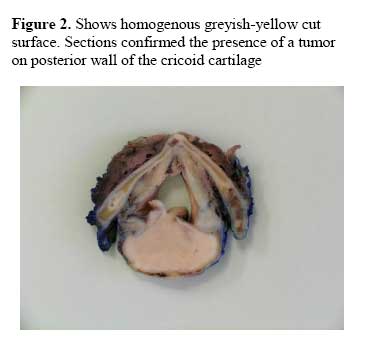
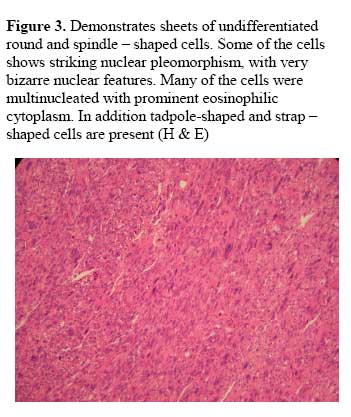
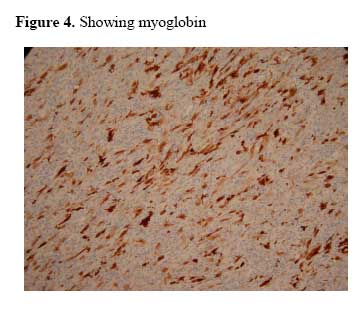
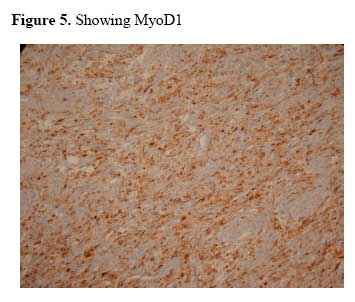
Kingdom Code Number: am07042 Abstract Rhabdomyosarcoma is relatively seen in the pediatric age group with the head and neck region as the commonest site. To the best of our knowledge, few cases of laryngeal involvement in adult have been described in the literature. Biologically, rhabdomyosarcoma is different from squamous cell carcinoma, which is the commonest tumor of the larynx. A previously healthy non-smoker 77-year-old lady presented to the ENT outpatient with a six weeks history of intermittent alteration of voice quality. She had no history of sore throat, or any symptoms suggesting laryngo-pharyngeal reflux. Examination showed asymmetry of the left arytenoid cartilage and aryepiglottic fold. She subsequently had a direct laryngoscopy and biopsy. Histology and immunohistochemistry examination suggested the diagnosis of mesenchymal neoplasm. Following discussion at MDT she subsequently had a total laryngectomy. Histology confirmed a completely excised laryngeal rhabdomyosarcoma. Rhabdomyosarcoma of larynx in adult is a rare disease. Surgical treatment with or without adjuvant radiotherapy is currently the treatment of choice for this disease. Key words: Rhabdomyosarcoma, larynx cancer Résumé Le Rhabdomyosarcome est relativement connu dans le groupe d’âge pédiatrique et les régions les plus touchées sont la tête et le cou. A notre connaissance, peu de cas de l’implication du larynx chez des adultes ont été cités dans la littérature. Biologiquement, rhabdomyosarcome est différent de la cellule squameuse carcinome, qui est la tumeur de larynx la plus ordinaire. Une femme non-fumeuse, âgée de 77 ans d’une très bonne santé au départ, s’est présentée à l’ORL ambulatoire avec une période de six semaines histoires de l’altération répétée de la qualité de la voix. Elle n’avait pas d’antécédente de maux de gorge ou aucun symptômes suggestifs le reflux laryngo-pharyngien. L’examen a montré l’asymétrie de la gauche aryténoïde cartilage aryepiglottique pli. Elle a par la suite eu une laryngoscopie directe et la biopsie. L’examen histologique et immunohistochimie a suggéré le diagnostique des tumeurs mesenchymteuses, néoplasme. A la suite d’une discussion au MDT elle a ensuite eu une laryngectomie totale. L’histologie a confirmé une excisée larynx chez des adultes qui est une maladie rare. Le traitement chirurgical avec ou sans radiothérapie adjuvante est actuellement le traitement du choix pour cette maladie. Mots clés: Rhabdomosarcome, le cancer du larynx Introduction Laryngeal cancer is an important cause of morbidity and mortality accounting to 25% of all head and neck cancers.1 The vast majority of laryngeal cancers are squamous cell carcinoma. Rhabdomyosarcoma is a malignant tumor of striated muscle rarely occurs in the larynx. In adults, rhabdomyosarcomas are extremely rare tumors, with few cases of these tumors have been adequately described in world literature in the adult population.2-4 There is very scanty literature on the presentation and behavior of laryngeal rhabdomyosarcoma. However because it is the most common malignant mesenchymal tumor in children,5 pediatric literature indicates that the most common site of presentation is in the head and neck region (35%). Lungs, bone marrow, bones, liver and brain are among the most common sites of metastases.6 Five years survival ranges from 30% in patients with metastasis at presentation to 80% in those where the disease is localized and complete resection is performed.4 It is unclear if rhabdomyosarcoma in larynx behaves similarly to those histologically different tumors occurring in other sites. Biologically, rhabdomyosarcoma is quite different from the more common cancer in larynx, which is squamous cell carcinoma. The diagnostic difficulties, immunohistochemistry and long term outcome of the various treatment modalities for adult primary laryngeal rhabdomyosarcoma are discussed. Case report A previously healthy non-smoker 77-year-old lady presented to the ENT outpatient with a six weeks history of intermittent alteration of voice quality. She had no history of sore throat or feeling of lump in throat, and had no symptoms suggesting laryngo-pharyngeal reflux. Initial examination with a flexible laryngoscope showed asymmetry of the left arytenoid cartilage and aryepiglottic fold. She subsequently had a direct laryngoscopy were an irregular swelling of the left arytenoid cartilage and left aryepiglottic fold was found. The tumor extended into the region of posterior comissure and adjacent cricoid cartilage. However the piriform fossa, vocal cords, epiglottis, valleculla, appeared normal. Biopsy was taken from the left arytenoids and aryepiglottic fold. CT scan of the larynx shows a bulky tumor involving the left arytenoid and post-cricoid cartilage. There was no nodal involvement and no evidence of metastasis on chest scan. The diagnosis of a mesenchymal neoplasm was made and following discussion at multidisciplinary team meeting (MDT), she subsequently had a total laryngectomy. (Figures 1 and 2) On immunohistochemistry the cells, demonstrated very bizarre staining for desmin and were strongly positive for vimentin, myoglobin and MyoD1. (Figures 3, 4 and 5) However they were negative for cytokeratin, EMA, CEA, S-100 protein and actin.There was no invasion of the underlying cartilage and the tumor was completely excised with a thin margin of about 0.5 mm. A diagnosis of completely excised laryngeal pleomorphic rhabdomyosarcoma was confirmed. She is been regularly followed up at the MDT Clinic, and she had no signs of local or regional recurrence over a year follow up. Discussion Rhabdomyosarcomas are mesenchymal tumors usually seen in children.4 Though in children it is reported to occur commonly in the head and neck region, the larynx is a very rare site even in this group.6 The literature on laryngeal Rhabdomyosarcomas indicates that in the larynx the tumor tends to originate in the vocal cord region and appear as polypoid mass, which may extend above and below the vocal cord.7 Presentation can vary from alteration in voice to a feeling of strange lump sensation in throat, or on rare occasions it may be life threatening because of upper airway obstruction.7 It is important to note that it’s presentation does not differ from the common presentations of squamous cell carcinoma, however they tend to grow rapidly and present with a short history of onset of symptoms.8 The challenge is to differentiate clinically benign from malignant lesions, when they present as a polypoid tumor. 7It is not clear if smoking plays any role in rhadomyosarcoma of the larynx. Our patient was a non –smoker. To the best of our knowledge, there is no association between smoking and rhabdomyosarcoma. Diagnosis is made from biopsy on direct laryngoscopy. CT scan is important in determining the extent of tumor. There are four main types of rhabdomyosarcoma. These are embryonal, alveolar, pleomorphic and botryoid. It is important to note that the pleomorphic type is uncommon in children and is rare, even in adults.9 Cross-striations are usually visible with ordinary hematoxylin-eosin staining accentuated by phosphotungstic acid – hematoxylin (PTAH) staining. Histologically tumor composed of sheets of anaplastic cells, several of the cells shows striking nuclear pleomorphism, with very bizarre nuclear features. Many of the cells are multinucleated with prominent eosinophilic cytoplasm. Tadpole-shaped and strap –shaped cells are commonly present (Figure 4).9 It is important to note that immunohistochemistry plays a key role in diagnosis. The tumor cells are strongly positive for desmin, vimentin, myoglobin and MyoD1, but negative for cytokeratine, epithelia membrane antigen, CEA, S-100 protein, and actin. MyoD1 RNA protein is highly sensitive and specific for rhabdomyosarcoma. 10 -12 Electron microscopic examination may be useful especially in uncertain cases.7 Treatment and prognosis is based on results of the Intergroup Rhabdomyosarcoma study group (IRS).13,14 Surgical treatment with adjuvant radiotherapy is currently the treatment of choice for laryngeal disease.2 However the use of adjuvant combination Chemotherapy with radiotherapy is gaining ground and reducing the need for mutilating surgery in head and neck rhabdomyosarcoma15,16; however it is not clear if this modality of treatment has any significant effect on outcome in adult laryngeal disease considering that only few cases has been reported. Improvement in outcome has been shown to occur with multimodality treatment regimens for head and neck rhabdomyosarcoma.17 Conclusion Rhabdomyosarcoma should be considered in any patient with a laryngeal polypoidal lesion and presenting with a very short history. References
Copyright 2007 - Annals of African Medicine The following images related to this document are available:Photo images[am07042f4.jpg] [am07042f5.jpg] [am07042f2.jpg] [am07042f1.jpg] [am07042f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}