 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
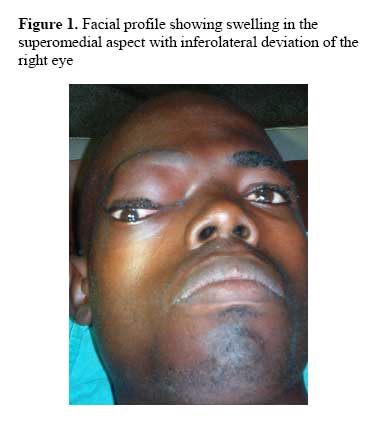
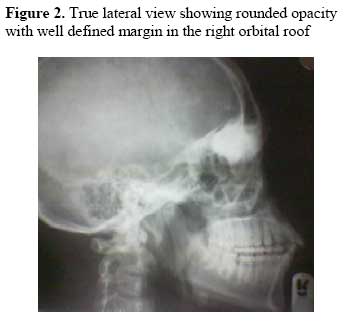
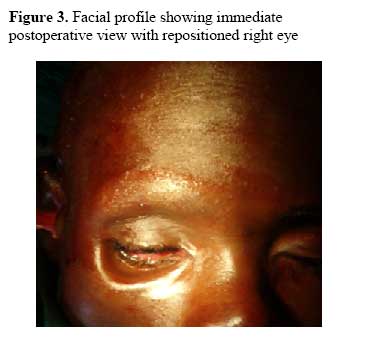
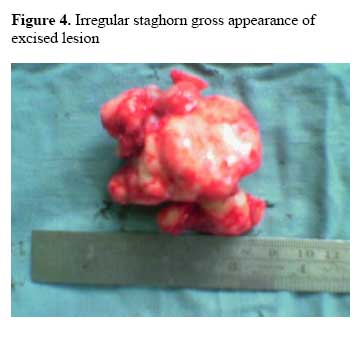
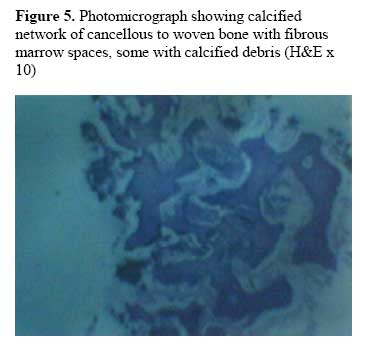
Annals of African Medicine, Vol. 6, No. 4, 2007, pp. 203 – 206 Myositis Ossificans Circumscripta of the Supra-orbital Region: A Case Report S. O.Ajike1, A.Mohammed2, E. T. O.Adebayo3, C. N.Ononiwu1, O. O.Omisakin4 1Department of Dental Surgery, Ahmadu Bello University, Zaria Nigeria Code Number: am07046 Abstract Myositis ossificans circumscripta is a pathological condition characterized by formation of bony tissue within the skeletal muscles following repeated trauma. A case of myositis ossificans circumscripta of the supra-orbital region in a 25-year-old man is presented and the pertinent literature is reviewed. To the best our knowledge this benign lesion has not been reported previously in the orbital region the world literature. Clinically the patient presented with a swelling and proptosis of the right eye. Radiologically there was a rounded opacity with well defined margin. Lesion was initially misdiagnosed as a fibro-osseous lesion; however microscopic examination indicated matured myositis ossificans. Lesion was excised via a bicoronal flap. Careful clinical, radiological and pathologic evaluation is required to make this uncommon diagnosis in an unusual location such as the supra-orbital region to avoid unnecessary surgical mutilation of the patient. Key words: Myositis ossificans, supraorbital Résumé La Myosite circumscripta ossificane est un état pathologique caractérisé par la formation de tissu osseux dans le muscle squelettique à la suite des traumatismes répétés. Un cas de la myosite circumscripta ossificane de la région supra orbitale chez un homme âgé de 25 ans est ici présenté et aussi la pertinence de la littérature est révisée. A notre connaissance, cette lésion bénigne n’a pas été signalée précédemment dans la région orbitale de la littérature du monde. Cliniquement le patient s’est présenté atteint du gonflement et du propose de l’œil droit. Radiologiquement, il y avait une opacité arrondie avec des marges bien définies. Lésion a été au départ mal diagnostiqué comme une fibro-lésion osseuse ; toutefois, l’examen microscopique avait indiqué la myosite ossification mûre. Lésion a été excisée par l’intermédiaire d’un bicoronal flap. Prise en charge clinique, radiologique et évaluation pathologique est nécessaire pour faire ce diagnostique rare dans une situation inhabituelle telle que la région supra orbitale afin d’éviter les mutilations chirurgicales évitable chez le patient Mots clés Myosite ossificane, supra orbitale Introduction Myositis ossificans circumscripta is a solitary non-progressive benign ossifying lesion.1 It is usually secondary to trauma2,3 or occasionally with no history of trauma.4 The pathogenesis of this lesion involves chipping of the periosteum, organization of hematoma with connective tissue metaplasia. There is no sex predilection, however, majority are reported in young adult males5 and less commonly in children.6 As the lesion progresses, plain radiographs will usually demonstrate floccullar opacification7 with no serum biochemical changes.8 Surgical excision is the main stay of treatment for myositis ossificans circumscripta.2,3,9,10 Previous reports of this pathology occurring in the head and neck region are case reports involving the temporalis5,9 and the masticatory3,10,11 muscles. We therefore present a case of limitation of ocular movement from myositis ossificans circumscripta in a very unusual location; the orbital plate of the frontal bone with no previous history of trauma. Case report A 25-year-old male farmer was referred with a history of swelling in the right supra-orbital rim and diplopia of two years duration. Swelling started as a small growth which was managed at a chemist shop with medications and massaging but still persisted. Past medical and dental histories were non-contributory. Maxillofacial examination revealed facial asymmetry with a swelling in the right supra-orbital region (Figure 1). There was proptosis, inferolateral displacement of the right eye with epiphora and diplopia of the right eye. Swelling was non-tender, bony hard with freely mobile overlying skin. Radiographic examination revealed a rounded opacity with well defined margin in the superomedial aspect of the right orbital rim (Figure 2). The paranasal sinuses were normal. A provisional diagnosis of fibro-osseous lesion was made; hematological test results and urinalysis were within normal limits. Under a nasoendotracheal intubation and after the routine cleaning and draping lesion was exposed and excised via a bicoronal approach and the resultant cavity was irrigated with normal saline. Hemostasis was achieved and a frontonasal drain was inserted. Flap was replaced and wound sutured with 1/0 silk. Immediate postoperatively the eye was repositioned in the socket with some degree of enophthalmos (Figure 3). Postoperative course was uneventful and there has been no recurrence 2 years after treatment. The excised lesion which measured approximately 7x5x4cm weighed 38g appeared as an irregular stag horn dense bony tissue covered by thin cartilage (Figure 4). Decalcified tissue on section, revealed a gray appearance with an irregular whiter central portion. Microscopy showed calcified network of cancellous to woven bone with fibrous marrow spaces, some with residual calcified debris (Figure 5). Discussion Myositis ossificans of the head and neck region is more commonly found in the masseteric,3 temporalis,5,9 buccinator,10 pterygoideus,11 sternomastoid12 and rarely in the scaleneus medius13 muscles. The case reported here was found in an unusual location; the orbital plate of the frontal bone. To the best our knowledge this may be the first case of myositis ossificans circumscipta to be documented in this location. Most authors have associated this lesion with trauma,2-6 however Ogilvie-harris4 documented a case without a history of trauma. In this reported case no history of trauma could be elicited. Occurrence of myositis ossificans usually results in functional impairments. In the masticatory muscles it results in trismus,3,5,11 in the sternomastoid muscles it leads to torticollis.12 In our case, there was restricted downward movement of the right eye with diplopia on downward gaze. This may be due to change in the configuration of the orbit and change in muscle fiber orientation due to the presence of the intra-ocular mass. This was corrected following surgery. Although, it may occur at an age with no gender predilection, it is rarely encountered in children6 and is more commonly reported in young adult males.5 This may probably be related to the implicated etiologic factor of trauma as males are more involved in physical activities. The biochemical findings are usually within normal limits. The erythrocyte sedimentation rate and white blood cell count are rarely elevated. This we believe further attests to the non-infective nature of this condition. Early radiographic examinations are usually unremarkable. This may masquerade as a cyst and in this our report a frontocele. However ultra-sound is a useful diagnostic tool at this stage.14 Serial radiographs are of immense value as this usually demonstrates the progression of the ossification at about two to six weeks from onset to circumscribed calcification at six to eight weeks.7 Computerized tomography scan demonstrates fascial edema and swelling in the earliest stage before ossification,14 while magnetic resonance imaging reveals variable heterogeneously enhanced mass in the muscles depending on the age of the lesion.15 Early stages of the lesion are usually misdiagnosed as osteosarcoma necessitating unwarranted radical surgery. Late stage myositis ossificans consisting almost entirely of mature lamellar bone, may be misinterpreted as an osteoma or a fibro-osseous lesion.6 Coincidentally, fibro-osseous lesion was the clinical diagnosis in this our report. The treatment of myositis ossificans is surgical excision13,15 of the lesion. The surgical approach of a bicoronal incision was to offer us a wide surgical field coupled with the absence of any facial scar or keloid post-operatively which is common in Africans. References
Copyright 2007 - Annals of African Medicine The following images related to this document are available:Photo images[am07046f2.jpg] [am07046f4.jpg] [am07046f5.jpg] [am07046f1.jpg] [am07046f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}