 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 7, No. 1, 2008, pp. 6-10 Adnexal Skin Tumors in Zaria, Nigeria M. O. A.Samaila Department of Pathology, Ahmadu Bello University Teaching
Hospital Shika –Zaria, Nigeria Code Number: am08002 Abstract Background: Adnexal
skin tumors share many features in common and differentiate along one line.
Their detailed morphological classification is difficult because of the variety
of tissue elements and patterns seen. They may be clinically confused with
other cutaneous tumors. The aim of this report is to review and classify all
adnexal tumors seen in a pathology department over a 16 year period. Key Words: Adnexal tumours, ecrine sweat gland Résumé Introduction:
Adnezal tumeurs de la peau partagent pas mal de traits caractéristiques en
commun et il y a des différences le long d’une ligne. Leur fiche de
classification morphologique est difficile en raison de la variété des éléments
des tissus et des tendances vues. Elles peuvent être cliniquement confondue
avec d’autres tumeurs cutanées. L’objet de ce rapport est de passer en revue et
de classifier tous les adnexal tumeurs vues dans un département de pathologie
au cours d’une durée de 16 ans. Mots clés: Adnexal tumeurs, eccrine glandes sudoripares Introduction The adnexae is part of the epidermis of the skin and is composed of different kinds of cells that can give rise to a wide variety of tumors.1-3 It is comprised of sweat glands, sebaceous glands and hair follicles, all of which share the same origin. Thus tumors arising from them share many features.1 Any detailed morphological classification of these tumors run into difficulties owing to the variety of tissue elements and patterns seen. The majority of these tumors are benign and are rarely malignant.4 This is a report of the histological patterns of adnexal tumors seen in a 16 year period. Materials and Methods All histologically diagnosed adnexal tumors at the department of Pathology, Ahmadu Bello University Teaching Hospital Zaria, Nigeria from January 1991 to December 2006 were reviewed. The tissue specimens were received and fixed in 10% formalin and were processed in paraffin wax. Histology sections stained with routine Haematoxylin & Eosin (H&E) were retrieved and reviewed by the authors. Special stains such as periodic acid schiff [PAS], Van Gieson and Alcian blue were employed where required. The biodata, clinical history and anatomical sites of lesions were obtained from patients’ accompanying case cards. The tumors were grouped based on adnexae origin. The most reliable histopathologic criteria for identifying malignant adnexal tumors are decapitation secretion, periodic acid schiff positive diastase resistant material in the cells and immunoreactivity with gross cystic disease fluid protein 15. Results There were 52 adnexal tumors. During the same period, a total of 5642 cutaneous tumors were seen. There were 26 males and females each, aged 4 days to 70 years (median -33 years). Two-peak age distributions (0-20 years and 40-50 years) were noted (Table 1). Duration of symptoms was from birth to 15 years (median 12 months). Clinical presentations included discreet swellings (15), nodules (23), hypertrophic surgical scar (1), polyps (6), ulcerations (3) and fungating masses (4). Five patients presented with recurrent lesions. Range of clinical diagnoses included pyogenic granuloma 4 (7.7%), papilloma 6 (11.5%), naevus 2 (3.8%), lipoma 3 (5.8%), hypertrophic scar 1 (1.9%), skin nodule 2 (3.8%), foreign body granuloma 1 (1.9%) molluscum contagiosum 2 (3.8%), chronic osteomyelitis 1 (1.9%), hematoma 1 (1.9%), fibroma 8 (15.4%), cysts 5 (9.6%), liposarcoma 1 (1.9%), rhabdomyosarcoma 1 (1.9%), malignant melanoma 6 (11.5%) and squamous cell carcinoma 6 (11.5%). Only two cases had a clinical diagnosis of syringoma. There was no positive family history of similar lesions in any of these patients. Tumors were categorized on adnexea origin: Sweat gland 41 (78.8%), sebaceous gland 7 (13.5%) and hair follicle 4 (7.7%). Forty-six (88.5%) were benign and six (11.5%) malignant (Table 2). Table 1. Distribution of 52 tumor and age
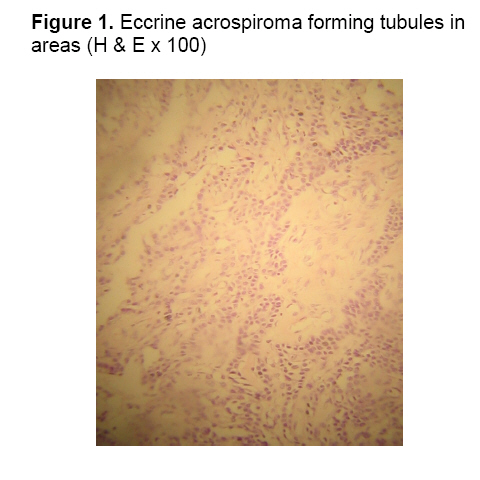
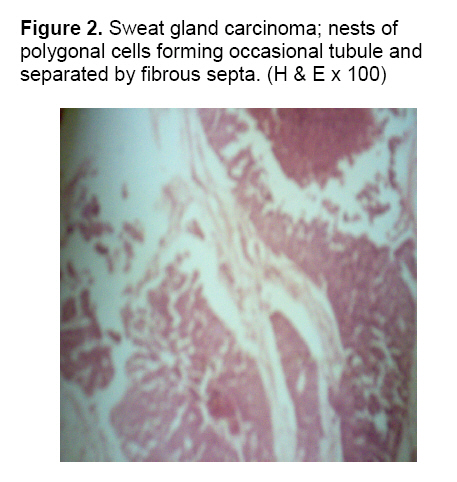
Sweat gland Benign sweat gland tumors comprised: eccrine acrospiroma 17 (32.7%), eccrine poroma 6 (11.5%), syringoma 5 (9.6%), eccrine dermal cylindroma 5 (9.6%) and papillary syringoadenoma 2 (3.8%). Eccrine acrospiroma was characterized histologically by solid nests of round to polygonal cells with clear to eosinophilic cytoplasm, forming tubules in areas (Figure 1). Distribution was mainly in the trunk and extremities. All five dermal cylindroma were confined to the scalp and microscopy showed tumor lobules composed of epithelial cell nests separated by hyaline material in a loose stroma. Malignant variant comprised eccrine sweat gland carcinoma (6; 11.5%) composed histologically of solid nests of large oval to spindle to polygonal epithelial cells forming occasional tubule containing eosinophilic globules and separated by fibrous septa (Figure 2). Sebaceous gland The sebaceous tumors comprised mainly a solitary sebaceous adenoma and six cases of nevus sebaceous of Jadassohn (NSJ). The NSJ showed immature sebaceous glands and pilar structures microscopically. Hair follicle Tumours of hair follicle included trichoepithelioma (3; 5.8%), characterized microscopically by multiple horn cysts and epithelial tracts connecting abortive pilar structures and a trichofolliculoma (1; 2%). Twenty-four (46.2%) cases were distributed between the scalp, face and neck, while 15 (28.8%) were distributed on the trunk. The trunk was also the commonest site for the malignant tumors. All sebaceous gland lesions were on the face (Table 3). Table 2. Distribution by of 52 tumors and sex
Table 3. Anatomical site of 53 tumors
Discussion Skin adnexal tumors constitute a small percentage of cutaneous tumors in our environment. They formed 0.9% of all cutaneous neoplasms seen in the Department during the study period emphasizing their rarity.2 No reliable data exist on the racial and geographic incidence of these tumors. Their causation is not well understood; however, the large majority differentiates along one adnexeal line.1,2 The sweat gland tumors were the largest group encountered in this study (78.8%). The complex nature of the sweat gland may be responsible for this wide array of tumors.1 Eccrine acrospiroma (hidradenoma) was in the majority with a wide age distribution from first to seventh decade and insignificant sex difference. The cases were distributed in nearly all the sites including hand, face, upper and lower limbs. The morphologic appearance was predominantly solid nests composed of round cells with dark nuclei and clear cytoplasm confined to the dermis, findings similar to other reports.2,5 Nevus sebaceous of Jadassohn is not neoplastic rather a tumor like lesion because of its harmatomatous conglomerate of sebaceous glands and heterotropic apocrine glands and defective hair follicle.1-4 The tumors of hair follicle, like those of sweat gland, have varying histological features than in their clinical features.2 The three cases of trichoepitheloma occurred as solitary tumors in the face, scalp and neck. None of the patients gave a positive family history. Solitary trichoepitheliomas, which are non-familial, may cause difficulty and are sometimes difficult to distinguish from a basal cell carcinoma. This confusion is understandable because of the linear differentiation of these tumors.1,2 Malignant adnexal tumors are rare world wide.4 The six cases encountered in the present report occurred predominantly in the trunk with a higher male frequency. One report noted the axilla as the preferred site.6 They represented 11.5% of the 52 tumors reviewed, further emphasizing their rarity. Malignant appendage tumors were the least common in one report,7 with four cases confined to the scalp and trunk and accounting for 3.3% of total tumors analyzed, and 2.3% in another report.8 Adnexal skin tumors have distinct histological patterns which differentiates them from other cutaneous tumors. They are commonly distributed in the head, neck and trunk. The commonest are benign variants from eccrine sweat gland origin and the malignant tumors are uncommon in our setting. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08002f1.jpg] [am08002f2.jpg] |
| |||||||||

{kind=link}
{kind=link}