 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
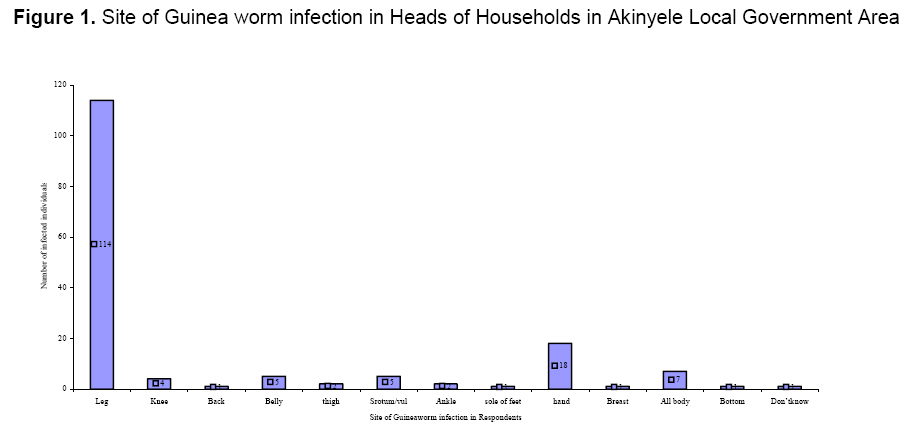
Annals of African Medicine, Vol. 7, No. 1, 2008, pp. 51-54 Letter to the Editor Perception and Management of Guinea Worm Disease In Infected and At Risk Non- Infected Communities in Oyo State, Nigeria O. A. Morenikeji and A. B. Odaibo Department of Zoology, University of Ibadan, Nigeria E-mail: jumokemorenikeji@yahoo.co.uk Code Number: am08012 Dracunculiasis or guinea worm disease caused by worm infestation continues to be a public health problem among rural communities in Africa, which depend upon unprotected water sources for drinking.Its health, social, educational and economic cost to the individual, the household and the community which is considerable and it’s transmission cycle are well documented.1,2 Key intervention strategies to eradicate guinea worm are safe water supply, vector control using abate, health education and case management. Besides the worm itself and the stagnant water/copepods combination, the third element in the cycle of the disease is the human being. This is probably the key element, for without the people’s cooperation and understanding none of the control strategies or intervention efforts will have much chance to succeed. The aim of this study therefore is to find out knowledge, attitude and practises (KAP) in the management of guinea worm disease in infected and at-risk non-infected villages. This study was carried out in12 villages in Akinyele Local Government Area (LGA) of Oyo State, Nigeria which lies between latitude 7°26/ 23// N to7° 40/ 30// N and between longitude 3° 47/ 4// E to 4° 05/ 00// E. Infected villages include these ones with their population at the time of study, Alagba (297),Oyeteju (45) and Olomitutu (215) while at-risk non-infected villages include Apapa (50houses), Alase (45houses), Ketepe (77), Deinlokun (25 houses), Aba Oso (56), Olorisaoko (55 houses), Alore (16 houses), Aroro (10 houses) and Ajibade (over 100 houses). Pretested and structured questionnaires were administered to all heads of households in infected and small non- infected villages while it was administered to every other house in bigger non-infected villages. The questions were translated into the language of the community, Yoruba. The questionnaire was used to record the demographic information of respondents. Source and treatment of drinking water, time of first infection, season, anatomical location, duration and severity of the infection were recorded. Effect of the disease on farming activities, information on the medication used and the knowledge of the disease were also recorded. Two hundred and sixty(260) households were sampled. 35.4% households in infected villages and 64.6% households in non-infected villages. 63.1% males and 36.9% females were sampled.80.8% were farmers. The number of respondents (75) that practice boiling and filtering of drinking water in infected villages is significantly higher than the number of respondents (32) that practice same treatment in non-infected villages(X2 = 95.5 ; P<.05) .Some respondents use alum as a preventive measure against guinea worm disease. 46.7% of the respondents from infected areas and 48.8% from non-infected areas had been infected before, 29.6% had their first infection as a child and had been re-infected many times. Most (68.8%) of the respondents were infected in the dry season. Most (91.2%) had the guinea worm coming out of their legs (Figure 1). Almost all the respondents (96%) had only one worm emerging at any one time. The period of disability in treated and untreated cases lasted from 1- 10 days to over a year. Table 1 shows symptoms perceived before bleb formation. 73.6% had their guinea worm ulcer healed within 1- 30 days. Most (81.6%) use palm oil for treatment. Herbs used include the traditional drug (agbo) made from boiled medicinal leaves (Olugambe leaves – Ipomea spp). Most of the respondents infected before (76%) could not farm at the time of infection and only 12% had alternative labor. Table 1 also shows that majority of the respondents from the infected villages (65.2%) and 66.1% from non-infected villages were ignorant of the fact that the guinea worm infection is caused by drinking contaminated water. When respondents were further probed,70.7% in infected villages and 76.8% in non – infected villages did not know guinea worm is transmitted in drinking water. 81.2% of the respondents from all areas believed that all ages are equally susceptible to infection. There is no significant difference between the number of people that know susceptibility is due to the use of bad water in infected and non-infected areas (X2 = 0.26;P>.05). 84.2% from all villages did not know if the disease is preventable or not. 64.4% said it could be treated using palm-oil. Majority of the respondents from all areas (77.3%) claimed to be doing nothing to control the disease in their houses. Of significance are the 10.4% that claimed to treat their drinking water for control. It is necessary to educate the villagers on the role of ponds as transmission sites, on the need to boil water and filter drinking water and the inability of the alum to kill the parasites intermediate hosts.. Educating villagers in all areas will help curb the menace of importation of the disease to at – risk non-infected areas where little or nothing is done about disease prevention. This study shows that guinea worm infection does not confer any tangible protective immunity on the patients. In this LGA where rainfall rises to a peak of 1000mm in the wet season, transmission is restricted to the tail end of the dry season. Patent guinea worm disease therefore reaches its peak in the following late dry season and early rainy season. Guinea worm came out mostly from the legs of those infected and most had only one worm emerging at any given time as found in studies by Kale.2 The older respondents recognized the prodromal signs of guinea worm infection. Use of palmoil, shea-butter and herbs for treatment of the disease in this study conforms to earlier studies.1 The long incubation period of the disease (9-12 months) makes it hard for people to visualize the direct connection between the water they drink today and the disease they suffer the following year. Table 1. Guinea worm infection in Heads of Households in Akinyele Local Government Area
Most(74.6%) of respondents interviewed did not know if the guinea worm is transmitted in drinking water or not which shows that water treatment was not done out of conviction. Some of the respondents never infected before claimed to have movement of worms all over their bodies. Respondents believe infection is not from drinking water because some people in the infected villages had never been infected before although born and lived all their lives there and because they feel it is either in the body, blood or a family disease of those infected. Those that said it is from drinking water stated it must be from a common source. When villagers’ minds are not set on getting rid of the disease, it might be difficult to eradicate the disease completely in the country. The location of boreholes and wells is not possible in all areas because of small population and topography of some areas. It will therefore be advantageous if health education is made to cover infected and at-risk non-infected areas in order to speed up the eradication of the disease. Acknowledgments This work was partly supported by UNICEF Southwest Zonal Office, Nigeria. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08012f1.jpg] |
| |||||||||

{kind=link}