 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 7, No. 2, 2008, pp. 62-66 Seasonal Variation in Admission for Heart Failure, Hypertension and Stroke in Uyo, South-Eastern Nigeria V. O.Ansa1 , J.U.Ekott2 , I.O.Essien2 , and E.O.Bassey2 1Department
of Medicine, University of Calabar Teaching Hospital, Calabar, Nigeria Code Number: am08014 Abstract Background: Seasonal variation in hospitalization for
cardiovascular disease has been described in the temperate regions of the world
as well as in Northern Nigeria. Increase admission rates during the cold
seasons have been reported in these areas. No studies have been done in
Southern Nigeria. This study is thus aimed at describing the seasonal variation
in admissions for heart failure, uncontrolled hypertension and hypertension
related-stroke in Southern Nigeria. Key words: Admissions, seasonal variation, cardiovascular diseases Résumé Culture générale: des variations saisonnières dans
l’hospitalisation pour les maladies cardiovascule ont été signale dans les
régions tempères du monde aussi bien que dans le nord du Nigeria. On a note une
augmentation d’hospitalisation dans ces régions pendant les saisons de pluies.
Aucune recherche n’a été faite au sud du Nigeria. Le but de cette étude est
donc de signaler les variations saisonnières dans l’hospitalisation des cas
comme ; insuffisance cardiaque, l’hypertension non maîtrisée et l’attaque
d’apoplexie lié a l’hypertension dans le sud du Nigeria. Mots clés: variation saisonnière, cardiovascule, hospitalisation Introduction Heart failure is a pathophysiological state in which there is impairment in the pump function such that the heart fails to maintain the circulation adequately.1 In nearly all regions in the world, heart failure is both common and on the rise.2,3 In Africa, at least 3%-7% of all hospital admissions are for heart failure.4 The cause of heart failure varies around the world, in sub-Saharan Africa including Nigeria, rheumatic heart disease is still a common cause especially in the young but hypertension is the major cause in the large cities.5 Other causes include dilated cardiomyopathy and its variant peripartum cardiomyopathy. Hypertension is largely asymptomatic and owing to the profound lack of awareness and poor perception of the disease, most Nigerian hypertensives frequently present in hospital only when complications occur or severely elevated blood pressure values incidentally recorded. Studies have demonstrated seasonal variation in the hospitalization for heart failure in the temperate climate.6-8 More admissions were found to occur in the cold (winter) season. A study in Northern Nigeria showed seasonal variation in hospitalization of cases of heart failure due to peripartum cardiomyopathy.9 Seasonal variation in arterial blood pressure has also been demonstrated among hypertensive patients in the temperate climate.10 A study from Northern Nigeria clearly showed an increase in hospitalization for hypertension-related morbidities in Sokoto during the cold seasons.11 In the southern states there are two distinct seasons, Wet (Cold) March to October and Dry (Hot) – November to February.12 Maximum temperature is between 31°C and 32°C with occasional extremes of 33°C to 34°C during the dry season. Minimum temperature ranges from 21°C to 23°C although sometimes figures as low as 18°C may be recorded in the wet season. This study is aimed at describing the seasonal variation in admissions for heart failure, hypertension and hypertension related stroke in a tertiary health institution in Southern Nigeria. Subjects and Methods Hospital records of patients admitted into the medical wards of the University of Uyo Teaching Hospital, Uyo (UUTH) with heart failure of all causes, uncontrolled hypertension and hypertension related-stroke (cerebrovascular accident) between January 1998 and December, 2001 were examined. Information extracted included age, sex, diagnosis and month of admission. The diagnosis of heart failure was made on the basis of clinical features and the specific etiological factors identified using hematological parameters, chest radiography, electrocardiography and 2D/M-mode echocardiography. Hypertension was diagnosed using the WHO/ISH criteria.13 A blood pressure of ≥ 140mmHg systolic and or 90mmHg diastolic was diagnostic. Stroke was diagnosed on the basis of clinical features only. Exclusion criteria:
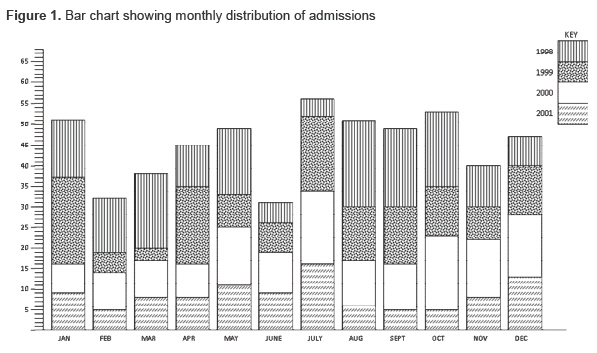
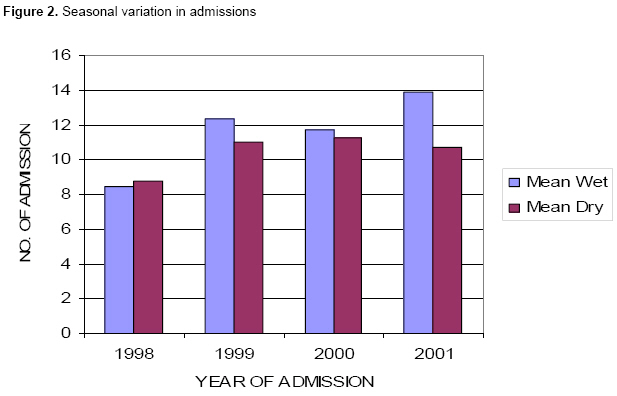
Data were analyzed in groups, means and percentages. The student t test was used to assess difference between groups. The level of statistical significance was fixed at P<.05. Results A total of 3550 patients were admitted into the medical wards during the study period. Of these 542(15.3%) were on account of heart failure of various causes, uncontrolled hypertension and hypertension related stroke. A breakdown showed that Heart failure accounted for 245(6.9%), uncontrolled hypertension 195(5.5%) and stroke (cerebrovascular accident) 102(2.9%). The study population comprised 300 males and 242 females. The ratio was approximately 1.2:1. Age range 18-94 years, with mean age of 52±12.8 years. Two hundred and forty five cases of heart failure (45.2%) were admitted, of these 90 (36.7%) were due to hypertension while 83(33.9%) were due to dilated cardiomyopathy. Anaemia and rheumatic heart disease accounted for 40(16.3%) and 32 (13.1%) respectively. One hundred and ninety five (36.0%) subjects were admitted for uncontrolled elevated blood pressure alone while 102 (18.8%) cases of cerebrovascular accident due to hypertension were admitted during the study period. The monthly distribution of admissions is shown in Figure 1. Monthly admission ranged from 5 to 21 with a mean of 11. Figure 2 illustrates the relationship between admission and the different climatic conditions. More admissions took place in the wet (cold) season than in the dry (hot) season. Table 1 shows comparison of admissions in the wet (cold) and dry (hot) seasons. It shows that even though there were more admissions during the wet (cold) season, the observed difference was only significant for heart failure and uncontrolled hypertension (P<.05) but not for stroke (cerebrovascular accident). Discussion Several studies on seasonal variation in heart failure hospitalization carried out in the temperate countries6-8 have shown an increase in admission during the winter (cold) season and a decline in summer (warm) season. Increase morbidity and hospitalization during cold season (Rainy/wet and Harmattan) due to heart failure caused by dialed cardiomyopathy as well as hypertension-related morbidities have been documented among Nigerians in the Northern part of Nigeria.9,11 This study from the southern part of Nigeria has demonstrated significant seasonal variation in hospitalization for heart failure and uncontrolled hypertension but not for cerebrovascular accident (stroke). Seasonal variation for stroke admissions has not been demonstrated here probably because of the small number of subjects with stroke recruited. Most patients with stroke do not get treatment in the hospital owing the traditional and spiritual beliefs that surround its etiology. The variation noted is despite the fact that during the two major seasons in the south (Rainy and Dry) extremes of temperatures are not usually recorded.12 Minimum temperatures in the south even in the wet season ranges between 21°C to 23°C with small diurnal variation. In the Northern part and plateau region, temperatures of between 9 and 18°C may be recorded in the cold season with large diurnal variation. Table 1. Comparison of admissions for cardiovascular disease during the dry (hot) and wet (cold) seasons
*Statistically significant The findings in this study may be explained by the fact that temperatures recorded in the south during the cold (wet) season are still low enough to trigger the cold induced changes in the cardiovascular system that would increase morbidity and thus hospitalization. These changes include increase in blood pressure consequent upon the thermoregulatory vasoconstriction. This is as a result of increase adrenaline and nor-adrenaline levels as well as an increase in peripheral resistance.13,14 Peripheral vasoconstriction induced by cold may also cause acute pulmonary edema by overloading the left ventricle particularly in those with hypertension.14 Modification of total extracellular volume is another mechanism. When temperatures decrease, loss of water by transpiration and perspiration decrease. These appear to be more important mechanisms of water loss than urine in patients with renal diseases and heart failure. Thus transpiration and perspiration may influence extracellular volume homeostasis in these patients than in normal subjects.15 Hospitalization for heart failure and hypertension therefore appears to more during the wet (cold) season in southern-Nigeria. Apart from the pathophysiological mechanisms outlined, the wet season is characterized by deterioration of the already bad road network which makes access to medical care difficult. Clinic appointments are not kept and compliance to medications poor resulting in clinical deterioration and complications warranting admission. Also, the intense agricultural activities during this season make patients and relatives not consider clinic visits a priority. Facilities and measures should then be put in place to receive and provide adequate medical care for these patients during this period of the year. A larger study involving more centers in the southern part of the country is indicated. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08014f1.jpg] [am08014f2.jpg] |
| |||||||||

{kind=link}
{kind=link}