 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
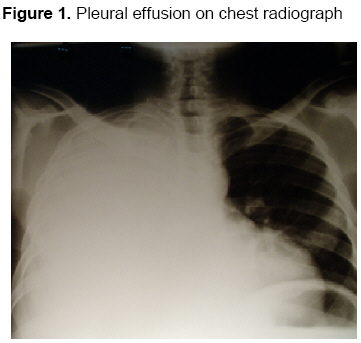
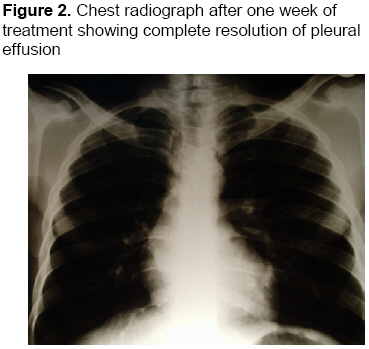
Annals of African Medicine, Vol. 7, No. 2, 2008, pp. 94-95 Letter to the Editor Hepatic hydrothorax with moderate Ascitis in a Nigerian S. B.Garko, O. S.David and M.Tasiu Department of Medicine, Ahmadu Bello University Teaching Hospital, P. M. B. 06, Shika, Zaria, Nigeria. E-mail: sbgarko@yahoo.com Code Number: am08022 Hydrothorax due to cirrhosis is usually right sided and has been attributed to defects in the diaphragm allowing the passage of ascitic fluid into the pleural cavity.1 Other suggested mechanisms include hypoalbimunaemia, hypertension in the azygous or hemiazygous systems and the presence of lymphatic channels in the diaphragm. A 34-year-old man with post hepatitic liver cirrhosis diagnosed in June 2005 was seen at our facility with a 3-week history of productive cough, orthopnea and chest pain. Had episodic exertional dyspnoea, parosxysmal nocturnal dyspnoea, painless bilateral leg swelling and no night sweats. He noted progressive abdominal swelling without associated abdominal pain or change in bowel habits. Examination confirmed cirrhosis with portal hypertension, right sided pleural effusion, moderate ascitis without asterixis. Chest x-ray confirmed pleural effusion (Figure 1). Repeated sputum acid-alcohol fast bacilli (AAFB) and culture were unremarkable. Liver function test showed marginal hypoalbuminaemia. A diagnosis of hepatic hydrothorax was made; He was started on treatment with salt restriction, injection intravenous frusemide, oral propranolol 40mg daily and oral augmentin 625mg 8 hourly. He was treated for a period of one week. He improved remarkably with total clearance of the pleural effusion (Figure 2). He was stable at 6 months of follow. Upto 5% of patients with cirrhosis and ascitis have an associated, usually right sided pleural effusion.2,3 Pleural effusion in cirrhosis without ascitis has been reported previously.2,4 The plausible pathogenesis is that, the cyclic negative intrathoracic pressures associated with respiration enhance the transdiaphragmatic migration of ascitic fluid into the pleural cavity. Mechanisms suggested for fluid passage into the thoracic cavity include: presence of a defect in the diaphragm, hypoalbuminaemia, hypertension in the azygous or hemiazygous systems and presence of lymphatic channels in the diaphragm. We could not establish a diaphragmatic defect in our patient due to lack of videothoracoscopy equipment. The transfer of fluid from the abdominal cavity to the pleural sac in the absence of cardiac or lung disease has been referred to as hepatic hydrothorax.5 Medical therapy includes salt restriction and diuretics. When these measures are ineffective, the patient has refractory hepatic hydrothorax.3 Our patient did well on medical management and did not re-accumulate at 6 months of follow up. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08022f2.jpg] [am08022f1.jpg] |
| |||||||||

{kind=link}
{kind=link}