 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 7, No. 3, September, 2008, pp. 112-119 Impact of Health Education on Home Treatment and Prevention of Malaria in Jengre, North Central Nigeria 1 O. O.Chirdan, 1 A. I.Zoakah, and 2C. L.Ejembi 1Department Of Community Medicine, Jos University
Teaching Hospital, Jos, Plateau State, Nigeria Code Number: am08026 Abstract Background: Malaria accounts for 1 million deaths among children
under five annually. It has been shown that improving home treatment and
preventing delays in seeking treatment, by teaching women to respond promptly
when their children have fever, can decrease malaria related complications and
mortality. This study looks at the impact of health education on knowledge of
malaria: its recognition, treatment and prevention among caregivers of children
under five in Jengre, North Central Nigeria. Key words: Health education, home treatment, malaria, prevention Résumé Contexte: Le paludisme occasionne chaque année 1 million de
décès chez les enfants de moins de 5 ans. Il a été démontré que l’amélioration
du traitement à domicile et le fait d’éviter le retard de prise en charge, par
des enseignantes afin de réagir avec promptitude lorsque leurs enfants ont la
fièvre, peut réduire les complications et la mortalité liées au paludisme.
Cette étude s’est intéressée à l’impact de l’éducation à la sante, sur la
connaissance du paludisme, son identification, son traitement et sa prévention
parmi les donneurs de soins aux enfants de moins de 5 ans à Jenre dans la
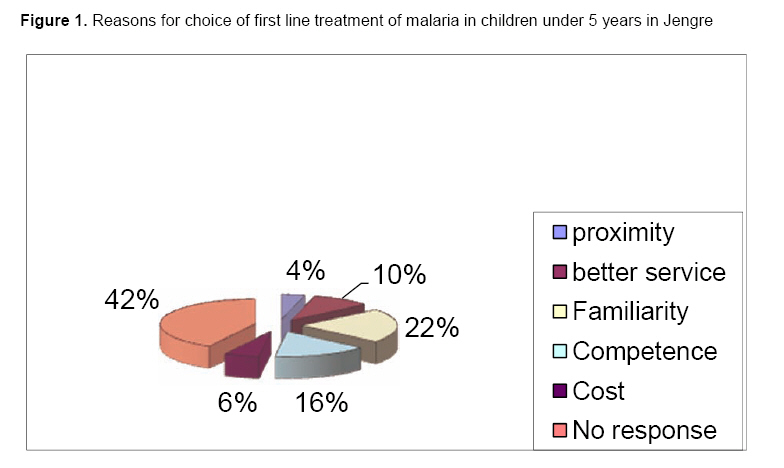
région du Centre-Nord du Nigeria. Most-clés: Education sanitaire, traitement a domicile, paludisme, prévention Introduction Malaria continues to present a great challenge to health systems for countries in the tropical developing world.1 In fact malaria affects many countries that are already under a heavy burden from the effects of HIV/AIDS. It is also responsible for 10% of hospital admissions and 20 – 30% of out patients’ consultations in Africa.2-5 In 1998, about 2400 million people in the world were at risk of malaria, with 300 – 500 million cases occurring globally each year; 90% of these are in Africa. It accounts for 1.1 - 2.7 million deaths worldwide annually and 1 million of these deaths are children under five living in Sub Saharan Africa. The case fatality rate for severe malaria among children is 10%-30%. The deaths are mainly due to anemia and cerebral malaria.2-5 Malaria is a common cause of fever in Nigeria. Fifty nine million people suffer from malaria each year. Children under five and pregnant women are worst affected. It is estimated that children under five years of age in Nigeria suffer 2 – 4 attacks every year, causing complications like cerebral malaria, severe anemia and death; and in some extent it impairs cognitive development, increases school absenteeism and is a major consumer of household funds.3,6 Early treatment, which is one of the cornerstones of malaria control in sub-Saharan Africa, depends upon prompt recognition of symptoms and signs at the home level. It is at this level that individuals and caregivers recognize illness and decide on treatment options. In Africa, home management of illnesses is very important and popular. It is the first line of treatment for many diseases including malaria. Reviews have shown that a large proportion of malaria treatment is done at home.7 The second line of action is usually sought only after home treatment fails. This is usually in public or private health care facility.7-16 In the rural areas, home management is usually opted for in form of self-treatment after a presumptive diagnosis of malaria is made. This self-treatment usually consists of antimalarials, antipyretics and herbs. The modern drugs were found to be more popular than the local herbs. The drugs are usually procured from the patent medicine vendors and drugs shops. 9, 10, 17. In Kabale, Uganda 53%,17 Western Kenya 60%,13,18 Butajira, Ethiopia 64.5%,9 Nigeria 70.5%12 Mali 75.8%,19 Bungoma, Kenya 47%,20 Zambia 80%11 and in Togo 83%13,14 were treated at home as first line action. Studies in Edu L.G.A., Nigeria and Lowveld area Swaziland showed a relatively high proportion of women using the health care facility (54%-86.1%).21 Studies have shown that majority of early treatment that occur in the informal health sector are usually inappropriate and sub–optimal.22-24 Mothers are primary caregivers and are usually the first to recognize signs of illness in their children. It has been demonstrated that educating mothers on malaria recognition and treatment can improve the effectiveness of malaria control programs.25 This study explored the responsiveness of mothers to information on home management and proper treatment seeking behavior about childhood fevers. This will provide information that will help reduce malaria related complications and mortality. Methodology Study Area Bassa Local Government Area (L.G.A.) is one of the 17 LGAs of Plateau state. The L.G.A was created in 1976; it is located on the Jos Plateau about 10km west of Jos, the Plateau State capital. The L.G.A. covers an area of 292 715sqm and has a projected population of over 160 000 people (based on local government targets). The L.G.A. is largely rural with its administrative seat in Jebu Bassa. Jengre is one of the major settlements in Bassa L.G.A. and has a population of about 31 200 (based on local government targets). people. It is located along the Jos-Kaduna highway; at the base of the Jos Plateau about 40km from Jos. The settlement falls within the Guinea Savannah Zone. The climate is typical of the rest of the Plateau, with a mean annual temperature of 20°C – 25°C. The mean annual rainfall is 146cm. April-October is generally warmer and this coincides with the rainy season. The harmattan period, December – February is much colder. The town is heterogeneous in ethnic makeup. The predominant ethnic groups are Amo, Jere, Lemoro, Gusu, Hausa-Fulanni, and Kuramas. Two health care facilities serve the town; one an L.G.A. owned Primary Health-Care (PHC) center and the other a mission hospital run by the Seventh Day Adventist Church. Two private clinics and 15 patent medicine vendors also serve the town. Study design The study was a community-based intervention, with data collected using quantitative methods, and had the following components: A baseline study to assess the perceptions, knowledge and malaria care seeking practices when children under five have fever. The use of the baseline data to develop and implement a community education program on malaria. A post intervention evaluation of the impact of health education using the same methodology. Baseline study Female caregivers of children under five years were studied. This group forms about 20% of the total population. Minimum sample size calculation was made to determine the size of this population. Sample size determination Sample size was determined using the p value of 54.3% of children with fevers were treated with the correct dose of chloroquine 23 in Edu L G A Kwara state in Nigeria 54.3% of children with fevers were treated with the correct dose of chloroquine . 23 The calculated minimum sample size was 150 women. Female caregivers of children under five. Sampling method A multistage sampling method was used. Stage 1 A list of settlements in Bassa L.G.A. was made and one settlement was selected by balloting Mapping of the houses and landmarks was done. Household numbering, listing and census were done A list of households containing children under five years of age was drawn. This formed the sampling frame. The total number of households forming the frame was 623. Stage 2 From this list 150 households were selected, with the aid of computer generated random numbers on EPI info 2000 statistical package. Only one eligible child per household was used in the study. A semi-structured questionnaire was interviewer administered. The respondents were female caregivers of children under five. The questionnaire was pre-tested on 20 women in Dilimi village, Jos East LGA. Questions that appeared ambiguous were re-phrased and repetitions removed. Intervention design The aims of the intervention are to strengthen the malaria knowledge, practice of prevention and treatment practice concerning malaria among caregivers of children under five. Targets Caregivers of children under five, who responded to the baseline questionnaire. An intervention was designed using the results from the baseline study. Training Health education training was done, targeting mothers of children under five and in Jengre. The 150 caregivers were grouped into 8 groups. The training was done at the waiting hall of the Primary Health Care facility (PHC) in Jengre. Two of the PHC staff was recruited to act as translators during the training. The training consisted of three sessions for each group of caregivers. Each training session lasted 45 minutes to one hour. The training guideline used was adapted from WHO Community health workers’ training manual.26 The training was divided into three parts: Part 1: What malaria is, its causation, transmission and its effects on the family, the community and the nation. Part 2: Recognition of uncomplicated malaria and severe malaria. Danger signs in children under five, action that can be taken at home and dangers of self treatment. Part 3: Treatment of uncomplicated malaria and prevention of malaria. Posters and chloroquine drug charts were used as teaching aids. Post intervention impact assessment All caregivers who attended the training were administered the same questionnaire used in the baseline assessment. Assessment of knowledge The responses of respondents to knowledge questions were scored. Each correct response received two marks while an incorrect response zero. All scores were summed. Respondents having scores of ≥50% of the total score were classified as having adequate knowledge. Those having scores <50% were classified as having inadequate knowledge. Results Baseline The respondents comprised of 150 women who were caregivers of children under five. Their mean age was 30±6.13 years (range 18-53 years). Sixty (40%) respondents were Amo (one of the minority ethnic groups found in central Nigeria) by ethnicity. Eighty (53.3%) and 32 (21.3%) of the women were housewives and farmers respectively. Forty-four (29.3%) had no formal education, 67 (44.7%) had some primary education while the rest had at least some secondary education The mean duration of formal education was 4 years (range 1 - 18 years). Malaria was recognized as one of the common and important diseases that cause fever in community by all the respondents. One hundred and fourteen (76%) could name at least 3 correct symptoms of uncomplicated malaria in children namely; fever, loss of appetite, chills and rigors, headaches. One hundred and four (69.3%) of the respondents knew that it was transmitted by mosquito. However, 95(62.7%) of the respondents did not know that malaria was caused by a blood parasite and did not know the exact relationship between malaria and mosquitoes. Sixty-one (40.6%) had adequate knowledge concerning malaria causation, transmission, prevention and treatment. Fifty (33.3%) children under five had fever in the two weeks preceding the baseline interview. The mean and median age of the children was 23 and 18 months respectively (±19.9 months). Twenty five (50%) of children who had malaria presented with fever and 11(22%) vomiting. At onset of the fever 16(32%) tepid sponged their children or gave an analgesic and 34 (68%) gave their children a cold bath, plenty of fluids to drink or did nothing. Self-treatment was the most popular first line of treatment optin 28(56%). Fourteen (28%) visited the patent medicine vendor (PMV), while eight (16%) visited the hospital. Mothers 19 (38.8%), fathers 8 (16.3%) and PMVs 11(22.5%) did the consultations. Health workers namely doctors, nurses and community health extension workers (CHEWs) consulted in 8 (22.5%). Reasons given for preferences included closeness to their dwelling, familiarity with person consulting, quality of treatment, perceived competence of person consulting and cost of treatment. Chloroquine syrup and injections were popular (Figure 1). Twenty five (51%) got better after the treatment while 24(49%) did not. The time interval between onset of illness and consultation was less than 8 hours in 34(68%), between 8 to 24 hours in 8(16%) and more than 24 hours in 8(16%). The second line of action in 12(50%) of the children was the hospital. The main reason given was perceived competence of the staff. Eleven (45.8%) visited the PMVs and 1(4.2%) used left over drugs. Regarding treatment seeking for children, the first action taken at home was significantly associated with caregiver’s knowledge of malaria (P=.018) (Table 1). Age of mother (P=.333), ethnic group (P=.313) and marital status (P=.064) was not associated with first action taken at home. A statistically significant association was found between years of formal education and first line treatment option. Women who had less than six years of formal education were more likely to engage in self-treatment of their children. Knowledge about malaria (P=.12), age of mother (P=.32), ethnic group (P=.77) and marital status (P=.332) was not associated with first line treatment option. The time interval between onset of fever and treatment was not associated with knowledge about malaria (P=. 88), age of mother (P=.08), ethnic group (P=.99) and marital status (P=.09). Personnel consulting and cost of treatment in the first treatment option was not significantly associated with knowledge about malaria (P=.33), age of mother (P=.33), ethnic group (P=.08) and marital status (P=.06). Child’s age was not significantly associated with treatment options (P=.07). Second line treatment option was significantly associated with caregiver’s knowledge (Table 2). There was no association between second line treatment and age of mother (P=.28), ethnic group (P=.22) and marital status (P=.06). Assessment of impact of intervention Statistically significant improvement was seen in thefirst action taken at home after the onset of fever, first line treatment option and treatment given (P=.03 and 0.04 respectively), (Table 4). The dosageof chloroquine given by the mothers did not changesignificantly (P=.33). Time interval between onset of fever and first treatment action did not change significantly (P=.51), (Table 3). There was significant change in second line treatment option (P=.02). Table 1. Relationship between care giver’s knowledge and first action taken at home
Chi square value=5.633, degree of freedom=1, P=.018 Table 2. Relationship between care giver’s knowledge and second line action
Chi square value=6.34, degree of freedom=1, P=.033 Table 3. Impact of health education on malaria treatment
CQ=Chloroquine; PCM= Paracetamol Discussion Caregivers acted promptly after the onset of fever. Among those that acted, only 48(32%) took an appropriate action, either tepid sponging the child or giving an analgesic. There was statistically significant relationship between malaria knowledge and first action taken at home. In majority of children, the mothers prescribed and purchased the antimalarials from PMVs. The reason given by majority of the women was proximity of the drug outlets to their homes and familiarity with the PMVs. Women who were aged 18-42 years were more likely to prescribe and buy drugs from the PMVs themselves, than visit the health care facility. The cost of antimalarials in the public health care facility was lower than the cost of antimalarials in the drug outlets. The private health care facilities were the most expensive. However, the PMVs were more popular as a first line treatment option and cost of treatment was not associated with choice of treatment options; hence proximity and familiarity may play a greater role in the choice of treatment option. The PMVs due to their familiarity with their customers allow customers to purchase drugs and pay in installments. They also allow customers to purchase part of the full treatment course when they are unable to pay for the full course. This is not possible in the public health facility. Findings from other studies showed that cost of treatment, waiting time and perception of severity of illness were factors associated with choice of treatment options.22,24-27 However, this study may not differ too much from other studies as reasons given can be explained along the same lines. ParacetamolR was the most popular analgesic while chloroquine was the most popular drug used in Jengre for treatment of malaria. Syrups and injectibles were preferred by the caregivers. Injection use was not high; this is similar to other studies.28-30 Pre-packaged forms of chloroquine were not available in any of the drug outlets in Jengre or any of the health care facilities at the time of the study. This is important as pre-packaging helps ensure adequate dosaging. Syrups are the most popular preparations used in Jengre for children and it has been associated with wrong dosages.31 It was observed that health facilities did not stock sulphadoxine-pyremethamine. Herbal preparations appear to be widely used for the treatment of malaria, though few caregivers acknowledged this. Eighty six percent of children with malaria were treated within 24 hours of onset of fever. This conforms to findings in other African studies.31 However only 32% of these treatments were with adequate dosage of chloroquine, and 24% of children treated in a health facility had the adequate dose of choloroquine. Treatment seeking behavior also improved. More caregivers visited the health care facility, more malaria episodes were treated with chloroquine after the intervention. However, the dose of chloroquine the caregivers gave their children did not change significantly. This suggests that there is a problem with caregivers administration of chloroquine. This agrees with findings from other research.32 The time interval between onset of fever and the first line treatment action did not change significantly: the women were acting promptly before the intervention. The study reveals that mothers, caregivers of children under five are responsive to information on home management of childhood fevers. This reveals opportunities that can be explored to improve child health and reduce malaria related mortality at community level. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08026f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}