 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 7, No. 3, September, 2008, pp. 120-127 Factors Influencing the Pattern of Self-Medication in an Adult Nigerian Population A. O.Afolabi Department of Dental
Services, Federal Medical Centre, Owo, Ondo State, Nigeria Code Number: am08027 Abstract Background: Despite
the growing research interest in self-medication, little information has been
available about its major determinants especially in developing countries. This
informed the conduct of this study to determine the major factors that
influence the pattern of self medication in a population of market women in
Ifako-Ijaiye area of Lagos, Nigeria. Key Words: Factors; pattern; self-medication; market women; Nigeria Résumé Contexte: Malgré l’intérêt croissant de la recherche sur
l’automédication, peu de connaissances sont disponibles sur les déterminants
majeurs notamment dans les pays en voie de développement. Cela est à l’origine
de cette étude ayant pour but de déterminer les facteurs majeurs influençant le
motif de l’automédication dans une population de femmes au marche dans la zone
de Ifako-Ijaiye a Lagos au Nigeria. Mots clés: Facteurs, Motif, automédication, femmes au marche, Nigeria Introduction The concept of self-medication which encourages an individual to look after minor ailments with simple and effective remedies has been adopted worldwide.1-3 People hold the view that medicine should be used in the event of any sickness or discomfort.4 In the United Kingdom where on the average 50% of health care takes place within the realm of self-medication, the government encourages self reliance,5,6 while agencies like the World Health Organization (WHO) promote individual family and community participation in primary health care.7 Poor diagnostic ability compounded by a limited knowledge of appropriate management result in the increase of self-medication and low rate of health care utilization.8 This shows that the practice cuts across culture, gender, health and social status, race, occupation or any other sociomedical or demographic factors. Many resort to the practice instead of contacting professional health care workers because of long waiting periods in hospitals,3 minor ailments,9,10 cost,11-13 to save money and time,14 lack of accessibility,11,15,16 shortage of doctors, or a feeling that their ailment is beyond the knowledge of western trained doctors.17 Individuals sometimes self administer medications through drug identification. Trade names were common means of identification and less frequently by generic name, action, color, shape and common usage names.18 Sources of drug information could be from the sales clerk in the chemist shop, 19 print media, family and friends, 20 pharmacists, general medicine dealers, general and private medical practitioners21 and among individuals who interact frequently with the public like hairdressers, salespeople and bank officials. Among the young ones, sources of drug knowledge include family members especially the mother (for therapeutic purposes), peer groups and the illegal market (for addiction purposes).22 Individual self-care in illness is shaped in the social environment - a major determinant of the type and amount of health care services used.23 The sociodemographic determinants are age, gender, occupation, educational level, marital status, religion, place of residence, race, income and culture. Despite the growing research interest in self-medication, little information has been available about its major determinants especially in developing countries.1, 24-26 Studies on factors influencing the pattern of this practice should be of interest to public health practitioners due to its possible deleterious effects especially in societies with high levels of illiteracy. Market women were chosen because the main providers of health care in the family are women, who often diagnose most common illness and treat them with the materials at hand. This informed the conduct of this study to determine the major factors which influence the pattern of self medication in a population of market women and to make rational recommendations. Methodology Ifako-Ijaiye local government was created on October 1996 out of Agege local government. Inhabited by over 266000 people according to 1991 census, majority of who belong to the Yoruba ethnic group. It is the most rural local government in metropolitan Lagos city, with nine known markets scattered within 11 wards. The study population consists of market women within the local government. Since there was no available literature showing the prevalence of self-medication among market women, a pilot study of 40 market women in Pen Cinema area of Agege, Lagos State, yielded a prevalence of 85%. This was used to determine the minimum sample size for this study using the formula27:
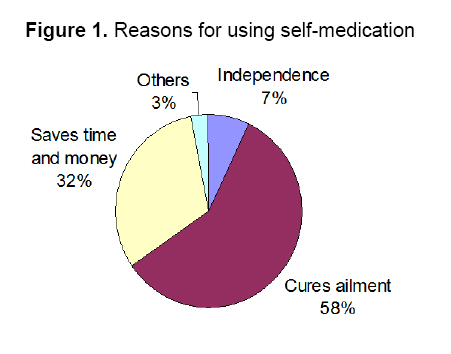
Where n = minimum sample size z = 1.96 at 95% confidence interval obtained from standard statistical table of normal distribution p = estimated prevalence of non-adherence in a given population (85% or 0.85) q = precision i.e. prevalence of adherence in a given population (1 – p or 0.15) d = margin of error (0.025) n = 196. With the minimum sample size known, a total of 205 market women were selected, using a multistage stratified sampling of the markets, stalls and finally market women (assuming a market woman per stall). Each of the nine markets was given a number and five were randomly picked: Ojokoro, Asokobowa, Ayewadun, Araromi and Baale-iju. These markets were enumerated for the total number of stalls (total of 475) and the market women selected by sampling fraction. From each of the selected stalls, market women were contacted, explanation about the purpose of the study was given, verbal and informed consent was granted before administering the questionnaire by the researcher and three trained assistants. Market women in this study are defined as those who sell goods in stalls, either open or locked-up excluding those who do not have a fixed location like local drug, wares, and alcoholic or herbal drink hawkers within the market. Study instrument was interviewer administered semi-structured pretested questionnaire with close-ended questions assessing major sociodemographic variables, how the medication was used, sources of information on medication used, where medication was obtained and benefits derived from self medication. Data obtained was entered into a micro computer running the statistical package for social sciences (SPSS version 12.0.1) soft ware to validate and analyze entries. Results of major factors influencing the pattern of self medication consist of generation of frequency tables and further analysis will explore statistical relationship between variables using χ2 test. The p-value will be set at 0.05. Results Of the 205 market women interviewed, with ages ranging between 15 to 65 years, the mean age was 34.2 years with standard deviation of 10.4 (Table 1). The modal age was 25-34 years and it accounted for 31.7% of the respondents. The response rate was about forty percent probably due to the less attention span of the market women because of anticipation of the next customer and considering the study of no financial advantage to them. Almost all the respondents (95%-98%) surveyed admitted one form of self medication or the other. Fifty-six point six percent (56.6%) of the respondents had at least a secondary school education while 23.9% and 19.5% had primary and no formal education respectively. Majority of the respondents (52.2%) were married, 20% were single, 14.2% were separated, 7.3% were divorced and 6.3% were widowed. Most of the market women sell foodstuff and vegetables (53.2%), provisions-milk, tea, sugar (17.6%), cosmetics (15.1%), clothes and bags (14.1%). Age and modality of use of medications (Table 2) Irrespective of the age group, most (66.0%) of the respondents used medications combined with each other rather than singly (34.0%). The prevalence was highest (72.1%) among the 34-44-year group and low in the extreme of ages: 59.5% among the 15-24-year group and 62.5% in the 54 years and above group. The association was not statistically significant. Age and source of information (Table 3) Patient Medicine Dealers were the most common (31.4%) single source of information on medications used followed by medical practitioners and other medical staff (20.6%), fellow market women (20.6%) and other sources - advertisement, family members, previous illness experience (27.5%). Source of information from patient medicine dealer was common among the older respondents (50.0% in the 45 – 54 age group and 62.5% in those 54 years and above). There was a negative correlation between sources of information through advertisement/mass media, family members, and previous illness experience with the age of the respondents. The association was not statistically significant. Education and the recognition of medications (Table 4) The commonest (61.1%) means of recognition was through trade and generic name followed by common usage names (21.7%) and color (17.2%). There was a positive correlation between recognition through trade or generic name and educational level of the respondents. It was 27.5% among those with no formal education (illiterates), 46.9% among the primary, 78.9% among the secondary and 79.2% among those with post secondary educational. On the other hand, most (45.0%) of the illiterates recognized their medications by color and 34.7% of those with primary education by common age names. The association was statistically significant. Education and where medication was obtained (Table 5) There was a positive correlation between the education level of the respondents and the tendency to obtain medications from the hospital/pharmacies. The prevalence among the illiterates was 7.5%, primary - 30.6%, secondary - 42.2% and post secondary education - 62.5%. In contrast, there was a negative correlation between the education level of the respondents and the tendency to obtain medications from patent medicine stores and local hawkers. For patent medicine stores, the prevalence was 75.0% of the illiterates, 53.1% of the primary, 46.7% of the secondary and 33.3% of the respondents with post secondary education. For those who obtained their medications from the local hawkers, the prevalence was 17.5% of the illiterates, 16.3% of the primary, 11.1% of the secondary and 4.2% of the post secondary educational level respondents. The association was statically significant. Marital status and where medication was obtained (Table 6) Most (54.7%) of the married respondents obtained their medications from patent medicine stones rather than hospital or pharmacies (32.1%) and local hawkers (13.2%). In contrast, hospital or pharmacies were the major source (61.0%) of medications for the single respondents compared to patent medicine stores (26.8%) and local hawkers (12.2%). In addition, 80% of the divorced, 76.9% of the widowed and 55.2% of the separated respondents obtained their medications from patent medicine stores respectively. Hence, the patent medicine store was the usual source (52.5%) of drug supply compared to hospital/pharmacies (34.8%) and local hawkers (12.7%). The association between marital status and where the medications were obtained was statistically significant. Benefits derived from self medication One hundred and eighteen (58.0%) of the respondents felt it cured their ailment, 65 (32.0%) said it saved time and money while 15 (7.0%) felt they had a feeling of independence to take care of themselves. Other responses accounted for the remaining 3.0% (Figure 1). Table 1. Characteristics of respondents
Table 2. Age and utilization of self-medication
* 2 non respondents. P>.05 not statistically significant Table 3. Age of respondents and sources of information on medications
* 1 non respondent P>.05 not statistically significant Table 4. Education of respondents and recognition of medications
*2 non respondents P<.05 statistically significant Table 5. Education of respondents and where medications was obtained
*2 non respondents P<.05 statistically significant Table 6. Marital status of respondents and where medications were obtained
*2 non respondents P<.05 statistically significant Discussion The study was carried out among market women most of whom were petty traders who sell foodstuffs and household items and are mainly of Yoruba ethnic group. This group of respondents is expected to share the same experience with respect to gender, occupation, race/tribe, socioeconomic status and income levels. Hence, an attempt was made to assess the effect of other factors like age, education and marital status on the pattern of self-medication. For all age groups, respondents used medications combined with each other rather than in single doses. Other studies reported similar findings.28, 29 The use of medications in combinations was low in the extreme of ages. This low prevalence among the elderly agrees with an earlier study30 while others16, 29, 31 reported high prevalence among the younger age group. Plausible explanation for the high used rate of medications consumed in combination among the 35-44year group might be due to the fact that these were the active group and tends to have more complaints, for instance, blood loss of menstruation, stress of daily market schedule and family problems, hence more drug use. The lowest used rate among the 15-24-year group might be attributed to their younger age; some may still be in school or learning a trade, low purchasing power and usually have less complaint. However, the fact that there was no association between age and self-medication agrees with previous studies.14, 32, 33 The finding that most of the respondents recognized their medications by trade or generic name was consistent with an earlier study.18 The positive correlation between education of the respondents and recognition of medication by trade or generic name could be due to the ability of the more educated respondents to clearly read the label on the medications consumed which may not be possible with those with little or no formal education. Therefore, those with little or no education recognized the medications more with their color and common usage names because they are easier to remember. The fact that majority (31.4%) of the respondents obtained information from the patent medicine dealers was consistent with a previous study.19 However as the respondents get younger, they tend to depend on other sources of information like mass media, adult family members, peer groups, advertisements and previous illness experiences. Possible reasons might be because the younger age group can easily be influenced through these means.21 Most of the respondents obtained their medications from patent medicine stores/dealers rather than the hospital/pharmacy or local hawkers. This is in contrast to other studies which mentioned local hawkers, 34 pharmacies1, 35 and general medicine dealers.36 There was a positive correlation between education and obtaining medications from hospital or pharmacy and a negative correlation with obtaining them from patent medicine stores and local hawkers. This finding is in agreement with previous studies. 13, 14, 37-39 This should not be surprising as the educated respondents might feel that the hospital or pharmacy have professionally trained personnel in terms of drug dispensing rather than patent medicine dealers who are not professionally trained. The finding that majority of the single respondents obtained their medication from the hospital/pharmacy rather than the patent medicine stores which was the common source for the widowed and divorced respondents might be attributed to their high literacy level compared to the widowed or divorced who are usually in the older age group where the literacy level is usually low. Hence, the single respondents would more likely visit the hospital/pharmacy rather than the patent medicine stores. The statistically significant association between the marital status and the practice of self medication was similarly reported.40, 41 In contrast; it is of minor significance in another study.42 This study revealed that the major factor which influences the pattern of self-medication among market women is education, either literacy or public. These groups of people require access to accurate and understandable information with regard to what each drug was meant for, and the potential benefit and risks associated with the use of such drugs including for self-medication purposes, provided in a language that can be understood, through the mass media and local government authorities. This information could involve highlighting management of common pathologies, when they should see a Doctor and problems that may arise from inappropriate medications and purchase of drugs from poorly trained individuals like local drug hawkers and patent medicine dealers. By regular education, this could have an effect on large sectors of the population, who, in turn, may directly influence their family and friends. Literacy education enables the individual to clearly read the labels on the medications consumed, thereby exposing them to the dose, duration, risks and side effects of the medications. In addition, as revealed from the study, the tendency to patronize local hawkers and patent medicine dealers decreases. The main channel of information and the usual source where medication was obtained were the patent medicine dealers, who are usually closer to the grassroots because of the limited number of Registered Pharmacist in a developing country like Nigeria. This study highlighted the importance of stricter control and regulation of the practice of patent medicine by the various State Ministries of Health, Pharmaceutical Society of Nigeria, and National Food and Drug Administration of Nigeria ensuring that only those that are genuinely qualified are issued license to practice, the practitioners knows their limitations as to what drug to dispense and when to refer to the hospitals. This will go a long way in preventing unnecessary adverse drug interaction, risks and side effects which could occur with the practice of self medication. Study limitations
Conclusion Literacy education of market women is invaluable. The study revealed that the more educated the market women become, the less she patronizes local hawkers or patent medicine stores. Literacy and public health education of market women should be carefully addressed by relevant government agencies. It is suggested that as part of the pet project of wives of State Governors in Nigeria, such program should be incorporated. After all, if you educate a girl-child, you educate a nation. Since the patent/general medicine dealers constitute the single substantial channel of information and the usual source where they obtain these medications, a forum or workshop should be organized for them regularly to update and improve their knowledge in managing simple complaints and dispensing OTC drugs. Recommendations
Acknowledgment I appreciate the hard work of my trained assistants, Mrs. Mary Afolabi, Mrs. Abiola Adojutelegan and Mrs. Oluyemisi Afolabi in data collection, without whose effort the study would not have been completed. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08027f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}