 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 7, No. 3, September, 2008, pp. 138-140 Case Report Pott’s Puffy Tumour: a Case Report B. B.Shehu and M. R.Mahmud Regional Centre For Neurosurgery, Usmanu Danfodio University Teaching
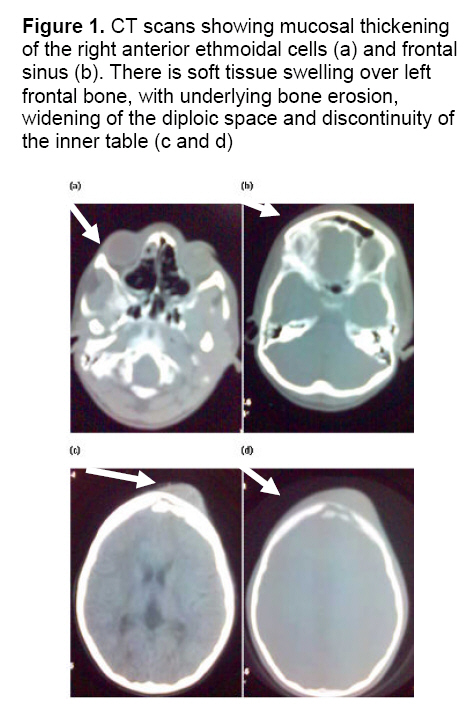
Hospital, Sokoto, Sokoto State, Nigeria Code Number: am08030 Abstract A 10-year-old girl presented with an episode of seizure following osteomyelitis of the frontal bone and subperiosteal abscess due to frontal sinusitis. CT scan confirmed osteomeyelitis of the frontal bone and subperiosteal abscess. At surgery, the subperiosteal abscess and contiguous subdural abscess was drained and sequestrectomy of the affected frontal bone done. Broad spectrum antibiotics and anticonvulsant were given for 4 weeks. The patient recovered without residual problems and has remained well at 5 years of follow up. Pott’s puffy tumor is now relatively uncommon and associated seizure is unusual. Early diagnosis and prompt treatment is necessary to avoid severe neurological complications and sequelae. Keywords: Pott’s puffy tumour, frontal sinusitis, seizure Résumé Une fille de 10 ans s'est présentée avec un épisode de la saisie après l'ostéomyélite de l'os frontal et de l'abcès subperiosteal dus à la sinusite frontale. Le balayage de CT a confirmé l'osteomeyelitis de l'os frontal et de l'abcès superiosteal. À la chirurgie, l'abcès subperiosteal et l'abcès subdural contigu étaient vidangés et sequestrectomy de l'os frontal affecté fait. De larges antibiotiques et anticonvulsant de spectre ont été donnés pendant 4 semaines. Le patient récupéré sans problèmes résiduels et est resté bien à 5 ans de suivi. La tumeur gonflée de Pott est maintenant relativement rare et la saisie associée est peu commune. Le diagnostic tôt et le traitement prompt est nécessaire pour éviter des complications et des conséquences neurologiques graves. Mots-clés: La tumeur gonflée de Pott, sinusite frontale, saisie Introduction Osteomyelitis of the frontal bone associated with subperiosteal abscess collection is termed Pott’s puffy tumour.1 Sir Percival Pott described this lesion in relation to forehead trauma in 1768, and in relation to early sinusitis in 1775. Pott’s puffy tumor is now relatively uncommon, 2 and complication with seizure is unusual. Case report A 10-year-old girl was referred to our unit with 3-month’ history of painful left periorbital swelling that was associated with photophobia, fever and headache, for which she received antibiotics and antimalarials at a peripheral hospital. The periorbital swelling persisted and 3 weeks prior to referral to us, she developed a painful left frontal swelling and had an episode of generalized convulsion. There was no preceding trauma and she had no history suggestive of sickle cell disease. On physical examination, temperature was 37.6°C, and there was no pallor. There was a tender, fluctuant swelling (4cm x 4cm) in the left frontal region with diffuse oedema and erythema involving the frontal and left periorbital. There were no focal neurologic deficits. White cell count was 11x109/L. Cranial computed tomography scan showed mucosal thickening of the right frontal and ethmoidal sinuses and soft tissue swelling over the left frontal bone. There were features of osteomyelitis of the frontal bone with sequestrum formation (Figure 1). Parenteral, broad spectrum antibiotics (ceftriaxone 50mg/kg body weight daily, and metronidazole 7.5mg/kg body weight 8hourly) and phenytoin (100mg 12 hourly) were commenced. At surgery, via a bifrontal scalp incision, subperiosteal and subdural abscess was drained and sequestrectomy of affected frontal bone done. Both aerobic and anaerobic culture of the pus was sterile. Post-operative course was uneventful. She was discharged after 5 days; the antibiotics were continued orally for 12 weeks and anticonvulsant for 18 months. She has remained well at 5 years of follow up. Discussion Since 1768 when Percival Pott described Pott’s puffy tumor a number of cases have been reported in literature. Though uncommon, the advent of antibiotics has not eradicated the disease, but has significantly reduced the incidence of major neurologic complications. It affects all ages from 7 to 83 years, predominantly teenagers. It is noteworthy that children suffer an average of 6 to 8 cold episodes per year, and 0.5% - 5% of these are complicated by sinusitis.3 Thus it is in this age group that major complications of sinusitis become a serious concern. Pott’s puffy tumour may follow trauma, but more commonly, it follows frontal sinusitis as in this patient. Infection extends from the frontal sinus through the frontal bone marrow cavity, causing osteomyelitis of the outer table, eroding it and causing subperiosteal abscess. The infection can also destroy the inner table resulting in an epidural abscess. Although the dura and arachnoid are relatively impermeable protective membranes, the infection can also spread to the subdural space causing subdural empyema or cerebritis, 3, 4 which manifests with seizure and neurologic deficits. Our patient had subdural abscess. Haematogenous spread via the valveless diploic veins may occur, giving rise to septic thrombophlebitis of the sagittal sinus, subdural empyaema and brain abscess. The most common pathogens implicated in Pott’s puffy tumour are non-enterococcal streptococci, staphylococcus, and anaerobes that colonize the upper respiratory tract.5 Gram-negative organisms are less frequently encountered. Cultures often reveal polymicrobial involvement. When intracranial complications occur, anaerobes such as fusibacterium, bacteroides, and anaerobic streptococci are the predominant pathogens. The presenting symptoms are commonly headache, periorbital swelling with erythaema, photophobia, preserved but discomforting ocular motility, and fever. Diagnosis should be suspected from clinical features of tender, fluctuant swelling over the frontal bone, but neuroimaging should be done to exclude intracranial complications. Plain and contrast enhanced cranial CT scan is accepted as the most adequate study, but magnetic resonance imaging, technetium-99m scan, and gallium-67 scan are also useful.6 Radiographic appearance in chronic osteomyelitis is that of a moth eaten appearance avascular necrosis, and presence of radio-opaque sequestra. Where sophisticated neuroimaging is not available, in terms of equipment or personnel, simple procedures such as skull x-ray may be performed. Radiographic evidence is seen only after 30 - 50% of bone is demineralised, and thus may be absent in the acute phase. This, however, will not conclusively show intracranial involvement.6, 7 The abscess should be drained and sequestrectomy of affected bone is important; this may be done endoscopically.8 Parenteral broad spectrum antibiotics are required and should be continued (orally) for 4 – 6 weeks to avoid recurrence. Anticonvulsants should be given in patients who have had a seizure and should be maintained for 12 – 18 months to avoid further seizures. Acknowledgment We are grateful to Dr (Mrs.). A. Umar of National Hospital, Abuja, Nigeria for radiological images and Dr. E. A. Ameh of Ahmadu Bello University, Zaria, Nigeria, for his useful comments. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08030f1.jpg] |
| |||||||||

{kind=link}