 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
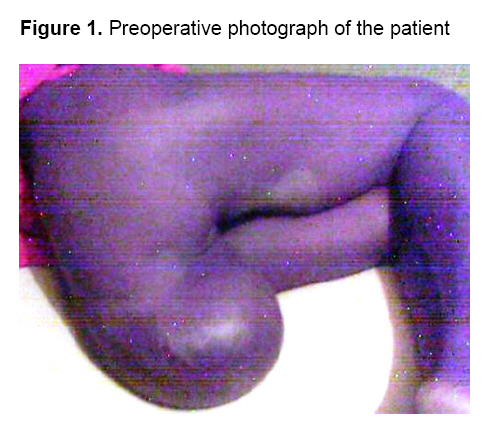
Annals of African Medicine, Vol. 7, No. 3, September, 2008, pp. 149-150 Sacrococcygeal Teratoma in an Adult Female Nigerian 1 K. N.Ozoilo, 2 M. G.Yilkudi and 1J. A.Ede 1Department
of Surgery, Dalhatu Araf Specialist Hospital Lafia, Nasarawa State, Nigeria Code Number: am08032 Sacrococcygeal teratoma (SCT), though rare, is the most commonly diagnosed childhood tumor, occurring in about 1: 40 000 live births.1,2 Said to arise from the primitive totipotent cells of Hensen’s node,3 it is usually diagnosed at birth because of its obvious nature and delayed presentations are unusual. It has a risk of malignant transformation that parallels the age of the patient. We saw a 45-year old female who presented with a swelling in the lower back since birth. It had grown considerably and prevented her from sitting erect. Initially painless, it had become painful following incision by a traditional blood letter, two months earlier. It was also discharging offensive fluid from the site of the incision. Two years earlier she had had an episode of pain for which she presented to a peripheral hospital. She was offered surgery then but declined. That episode resolved spontaneously and she had been symptom free untill the present episode. She was married and had ten children. Physical examination revealed a middle aged female in painful distress. There was a sessile mass attached to her sacrum and projecting down like an extra appendage (Figure 1). It was tender, cystic in some areas and hard in others. A shallow ulcer on the apex exuded clear offensive sero-purulent fluid. The anal orifice was displaced anteriorly but the sphincter was intact. There was no intra-rectal extension of the mass. There were no motor or sensory deficits in the lower limbs. Hematocrit was 37%, serum electrolytes and urea were within normal range and pelvic x-ray showed a soft tissue mass with no calcifications and no bony abnormalities. She could not afford pelvic ultrasonography,α -fetoprotein or β- HCG assays. With a working diagnosis of infected sacrococcygeal teraroma, she was commenced on broad spectrum antibiotics and offered excision biopsy. At surgery, the tumor was dissected completely with excision of the coccyx. The displaced anal orifice was repositioned and the wound closed over a closed suction drainage. Post operatively, the patient developed superficial wound infection which resolved on antibiotics and sitz baths. She was discharged on the 14th day post operatively but never attended any outpatient follow up. She was also discovered not to have sent the specimen for histology as instructed. Sacrococcygeal teratoma is usually diagnosed at birth because of its obvious nature. The tumor can grow to quite considerable proportions and the mature teratoma may possess digits and assume the appearance of a third leg projecting from the sacrum.4 The high risk of malignant transformation makes adult presentation particularly unusual, 5 but it is reported from time to time. Our patient had lived all her life, marrying and bearing children despite her obvious anomaly. Although the clinical examination and intra-operative findings seemed to suggest a benign tumor, the histology report would have afforded us a definitive diagnosis. The role played by poverty and ignorance in our patient’s case needs emphasis. She had a fairly balanced family and social life, not unduly concerned with the abnormality which protruded like an extra limb from her behind. She was unaware of the threat that a malignant transformation posed to her life with the progression of time. Only the unbearable pain and offensive discharge of infection forced her to seek and accept treatment. We recommend that enlightenment campaigns be mounted about congenital anomalies educating people about their causes, effects, management and prevention. The target audience would mainly be rural dwellers especially in the ante-natal setup. These campaigns could be incorporated into already existing maternal and child health programmes. We also urge clinicians to take the pains to educate patients in greater detail about their conditions at every opportunity. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08032f1.jpg] |
| |||||||||

{kind=link}