 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 7, No. 4, December, 2008, pp. 187-191 Meconium Peritonitis in Nigerian Children 1A. M.Abubakar, 2M. A.Odelola, 2 C. O.Bode, 3 A. O.Sowande, 4 M. A.Bello, 1 J. Y.Chinda and 5I.Jalo 1Paediatric
Surgery Unit, Department of Surgery, University of Maiduguri Teaching Hospital,
Maiduguri, Nigeria This paper was presented at the 5th Association of Paediatric Surgeons of Nigeria (APSON) annual scientific conference, Zaria, Nigeria 1st -4th November, 2006. Code Number: am08038 Abstract Background: Meconium peritonitis is a rare disease with a fatal
outcome. In Nigeria and Africa, there are only the occasional case reports on
the subject matter. Key words: Meconium, peritonitis, antenatal diagnosis, Hirschsprung’s disease, outcome Résumé Contexte: La péritonite à méconium est une maladie rare
d'issue fatale. Au Nigéria et en Afrique, seuls quelques cas cliniques se
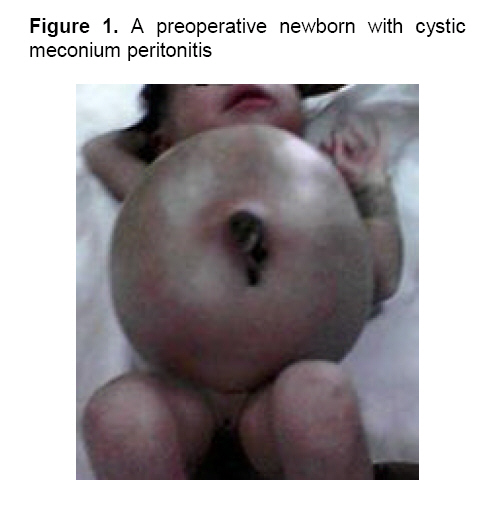
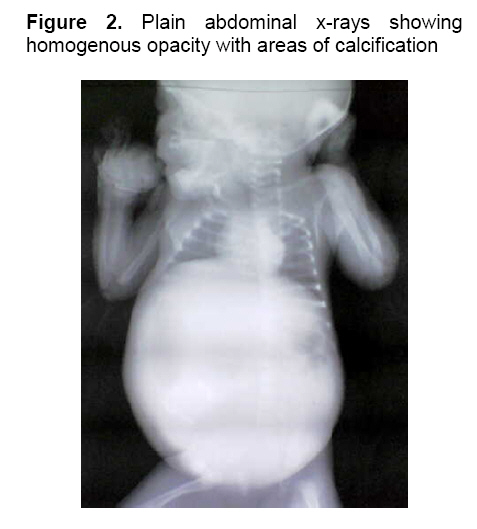
rapportent au sujet. Mots clés: Péritonite, méconium, diagnostic anténatal, maladie de Hirschsprung’s, prognostic Introduction Meconium peritonitis (MP) is a sterile chemical peritonitis resulting from perforation of the bowel inutero. Among neonates the incidence is 1:35 000 live births in the United states of America.1 In most cases the perforation occurs before an obstruction2 but obstruction may be absent.3 Other rare causes of MP include perforation of Meckel’s diverticulum, rectal perforation, perforated intestinal duplication, fetus-in-fetu and perforations caused by parvovirus B19 infection.4-7 Early diagnosis and prompt surgical intervention is critical to survival in these patients. The mortality rate becomes very high when they were operated on after the first 24 hours of life.4,8 In Nigeria9,10and Africa7,11 there is paucity of literature on MP as all were case reports. This is a multicenter study on all cases of MP presenting to us with highlights of the peculiar presentation and outcome of treatment. This is also an addition to the World literature on this rare problem. Materials and Methods A retrospective study of all patients with MP treated at the University of Maiduguri Teaching Hospital (UMTH), Maiduguri, Borno State, Lagos University Teaching Hospital, Lagos State(LUTH), Obafemi Awolowo University Teaching Hospitals Complex(OAUTHC), Ile-Ife, Osun State and the Federal Medical Centre Gombe(FMCG), Gombe State, Nigeria between January, 1998 and December, 2007. Data retrieved from the case files included the age at presentation, sex, place of birth, antenatal care, clinical presentation and investigations findings. Others included operative findings, operative procedures carried out, post-operative complications and outcome of treatment and follow up. The results are presented as simple percentages. Results Details of the results are summarized in Table 1. There were 10 neonates comprising 6 girls and 4 boys. The median age at presentation was 4 days (range 2-6 days). Six of the mothers of the children had supervised antenatal care with 4 having had an antenatal ultrasound examination but MP was missed in all these cases. Delivery was unsupervised at home for six of the mothers and in 4 of the mothers the delivery was in the hospital. The commonest clinical presentation was abdominal distention at birth in 9 of the 10 neonates (Figure 1). Others were failure to pass meconium in 5 patients, vomiting in 3, and fever in 2 patients and jaundice in one. Radiographic evidence of intraperitoneal calcification and homogenous opacity was present in 4 patients (Figure 2) and in 2 patients there was air under the diaphragm. At laparotomy, the findings were the generalized type in 7 patients, giant cysts in 2 and fibro adhesive in one patient. The commonest site of perforation was the terminal ileum (4 patients), others were the jejunum in 3 patients, cecum and splenic flexure of the colon in 1 patient each. In one of the patients the perforation had sealed at the time of surgery. The commonest causes of MP were intestinal atresia in 3 patients and Hirschsprung’s disease (HD) in 3 patients. One of the neonates had a high anorectal malformation (ARM). The remaining 3 patients had no identifiable cause. The procedures performed were resection and anastomosis in 5 patients and in one of these patients with resection and anastomosis there was an anastomotic dehiscence and an ileostomy was done. Simple closure and colostomy formation was carried out for 3 patients. Simple closure, cyst excision and drainage only were the procedures for one patient. Five of the 10 patients died in the immediate post-operative period. The patient on ileostomy defaulted after 2 visits on discharge. Only 4 of the 5 survivors were available for follow up for duration of 2 to 48 months. Table 1. Patients characteristics, etiology, operative findings, procedures and outcome of treatment
A: University of Maiduguri Teaching Hospital; B: Lagos University Teaching Hospital; C: Obafemi Awolowo University Teaching Hospital; D: Federal Medical Centre, Gombe; HD: Hirschsprung’s disease; ARM: Anorectal malformation Discussion Meconium peritonitis is a sterile chemical peritonitis resulting from antenatal passage of meconium from the fetal gut into the peritoneal cavity. It is rare with an incidence of 1:35 000 live births in the United States of America.1 In Nigeria9,10 and Africa7,11there had been only the occasional case reports on the subject of MP. In our series as in others intestinal obstruction is mostly responsible for MP4,8 and ileal atresia or meconium ileus is the major contributor to the intestinal obstruction. Intestinal atresia and Hirschsprung’s disease were responsible for MP in more than half of our cases, intestinal atresia was also the commonest cause of MP in a large series from South Korea.12 In the remaining patients, the etiology was unknown as no pathology was found. This is not unusual as absence of definite pathology has been documented by earlier reports.4,13 All these patients with no demonstrable pathology in our series were subjected to a rectal biopsy to rule out HD. Among Caucasians, meconium ileus is the commonest cause of MP and is present in 40% of postnatal cases.1 None of our patients as in the series of Nam and colleagues12 had features suggestive of meconium ileus even though no screening tests were carried out for cystic fibrosis as this is extremely rare in our practice. The clinical presentation is that of intestinal obstruction rather than peritonitis.4 However, rarely it may present as scrotal mass with calcification10 as seen in one of our patients. Other rare forms include passage of meconium through the vagina without an associated anorectal malformation or through the umbilicus.10,14 Antenatal sonographic diagnosis after the 24th week of gestation is now possible.15,16 In fact in a particular case some authors actually observed the leakage of meconium in the fetus during an ultrasound examination.16 Prenatal diagnosis will facilitate perinatal management by allowing for surgery as soon as possible after birth following resuscitation,17,18 thus avoiding the bacterial colonization that occurs after birth. This has led to reduction of operative mortality to about 2.4 to 23 per cent,4,12,16-18 when compared with the high rates in the early 1950s.4 Only half of our patients had a supervised antenatal care with an ultrasound examination. Meconium peritonitis was however, missed in all these cases. The implication is that the presentation to hospital is delayed with advanced disease and this is associated with the poorer outcome observed in our series. It will be expected that the rarity of meconium ileus will confer a better outcome as is the experience of people where this is also rare.12 A two staged approach with an initial enterostomy and subsequent reversal is generally advocated and has contributed to the reduction of the operative mortality.4,17 However, in our setting where facilities for neonatal intensive care and total parenteral nutrition are lacking and most patients come from poor backgrounds, multiple surgical operations within a short time span can be quite challenging. We have highlighted the peculiar features of this disease in some parts of Nigeria. In cases where there are no obvious causes for MP, a rectal biopsy is recommended to rule out HD. We hope that this report will facilitate early diagnosis of MP by sensitizing physicians to consider it as a differential diagnosis in any child with abdominal distension at birth. With proper operative procedure and meticulous post-operative care their survival should improve. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08038f1.jpg] [am08038f2.jpg] |
| |||||||||

{kind=link}
{kind=link}