 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Annals of African Medicine, Vol. 7, No. 4, December, 2008, pp. 200-204 Opinion Management Of Appendiceal Mass E. S. Garba and A.Ahmed Division of General Surgery, Department of Surgery, Ahmadu Bello
University Teaching Hospital Zaria, Nigeria Code Number: am08041 Abstract Background: The management of appendiceal mass is surrounded with
controversy. Traditional management has been conservative, with interval
appendicectomy performed weeks after the mass had resolved. This remains the
most common approach at many centers in the world. Recently, an increasing
number of studies have challenged this approach. This article reviews some of
the controversial issues in the management of appendix mass, assesses current
practice and suggests an appropriate approach for the management of appendix
mass. Keywords: Appendiceal mass, appendix abscess, appendix phlegmon, appendicitis, interval appendicectomy Résumé Contexte: La prise en charge du plastron appendiculaire est
entoure de controverses. Le traitement usuel a toujours été conservateur avec
l’appendicectomie réalisée plusieurs semaines après la fonte de la masse. C’est
l’attitude la plus commune dans la plupart des centres à travers le monde.
Récemment, un nombre croissant d'études ont conteste cette approche. Cet
article passe en revue certaines controverses dans la prise en charge du
plastron appendiculaire, présente les pratiques actuelles, et suggère une
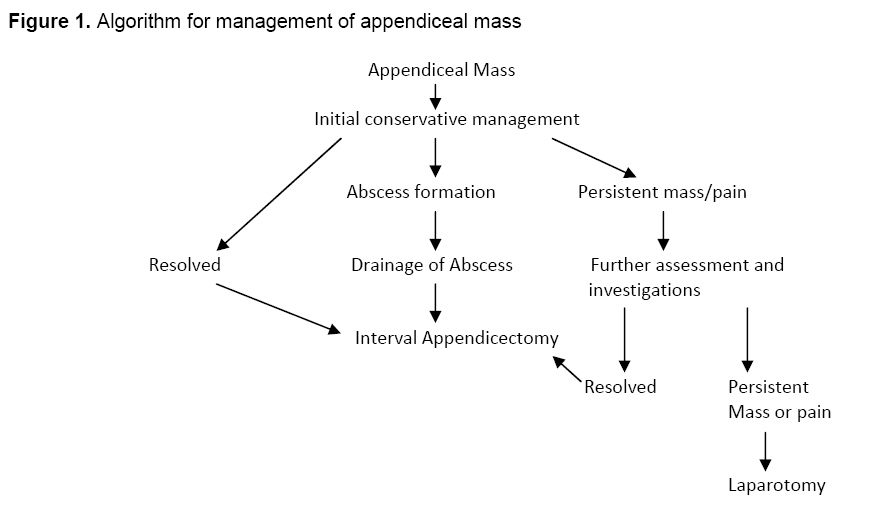
approche appropriée de la prise en charge du plastron appendiculaire. Mots clés: Masse appendiculaire, abcès appendiculaire, phlegmon appendiculaire, appendicite, appendicectomie a distance Introduction An appendiceal mass is the end result of a walled-off appendiceal perforation and represents a pathological spectrum ranging from phlegmon to abscess.1,2 It is a common surgical entity, encountered in 2%-6% of patients presenting with acute appendicitis.1-3 Management of an appendiceal mass is controversial with three general approaches usually employed.2-29 'Classical management' involves initial conservative management with broad-spectrum antibiotics and intravenous fluid until the inflammatory mass resolves. Patients are offered interval appendicectomy following resolution of symptoms. More recently, the need for interval appendicectomy has been questioned, with a number of authors adopting semi conservative approach with immediate appendicectomy or entirely conservative approach without interval appendicectomy.4-6. The semi-conservative approach involves performing immediate appendicectomy during the initial admission after resolution of the inflammatory mass. Advocates of immediate appendicectomy mentioned advantages of avoiding the need for readmission for interval appendicectomy, and the exclusion of other pathologies masquerading as an appendix mass.4-7 while advocates of interval appendicectomy described the advantages of avoiding recurrence of symptoms and the misdiagnosis of an appendix mass.8,9 They argue that interval appendicectomy is a less hazardous and less challenging operation, compared with immediate appendicectomy during the initial admission.8,9 Proponents of an entirely conservative approach claim appendicectomy, whether interval (delayed) or immediate (during initial admission), is unnecessary.10-12 None of these three approaches has gained total universal acceptance. At our center at Ahmadu Bello University Teaching Hospital Zaria, a classical approach is still favored by the majorities of the consultants (personal communications). This article aims to review the current available literatures describing management of appendix mass and suggest an acceptable approach based on available local resources. Materials and Methods A Medline, Pubmed and Cochrane database search was performed using reference manager 11 applying search key words such as: appendicitis, appendiceal mass, interval, appendicectomy, abscess and phlegmon. We also searched with the combinations of these key words using Boolean approach. Relevant articles including case series, review articles and individual case reports relating to adult appendix mass were selected and saved into the reference manager 11. Cases of children appendiceal masses were excluded from this review. All articles were read by the two authors and cross-referenced. Discussion An Appendiceal mass range from phlegmon to abscess and it develops in 2%-6% of cases following acute appendicitis2, 9-16. For obvious cases of appendiceal abscesses, there is no controversy as regarding its management; immediate surgical drainage (percutaneous or open) is the treatment of choice by the majority of the authors of the articles reviewed.6 For phlegmon, a number of treatment options ranging from conservative to aggressive approaches are available. We compared the three most popular approaches to the treatment of appendix mass. This discussion shall be grouped under the three main methods of approaches to treatment of appendix mass. Approach A Initial conservative treatment followed by interval appendectomy six to eight weeks later Oschner in 1901 proposed non-operative management for treatment of appendix mass.15, 16. This approach involved the administration of intravenous fluids and antibiotics while keeping the patient on nil per oral. The aim of this approach was to achieve complete resolution of the inflammatory mass and the disappearance of symptoms in the patient before any surgical intervention (Figure 1). Some authors favor this approach on the ground that it is effective in the majority of patients.16-18 What are the reasons for justifying interval appendicectomy? It is first to prevent recurrence of acute appendicitis and second to avoid misdiagnosing an alternative pathology such as malignancy.12,14,16 An article in favor of initial conservative approach published in 1993 by Nitecki et al2 reported a mean incidence of recurrent acute appendicitis in a meta-analysis of 329 patients managed conservatively as 13.7% (range 0%-20%).14 Most recurrences occurred within the first two years. There were also fewer operative difficulties in this group of patients and there was a far less frequent need to extend the incisions during surgery. As a result of these peculiar advantages the operative time was significantly shorter than other methods of treatment. There was also no significant postoperative complication in this group. Approach B Immediate appendicectomy following inflammatory mass resolution With the advent of antibiotics designed to prevent the growth of anaerobes, early appendectomy can now be carried out without complication19 Hence emergency appendicectomy for appendix mass is emerging as an alternative to conventional conservative treatment. It is said to be feasible, safe, and cost-effective, allowing early diagnosis and treatment of unexpected pathology.18 However, the appropriate timing for emergency surgery is contentious.18 One method involves immediate appendicectomy as soon as there is resolution of the mass before patient is discharged home during the initial admission. However some more aggressive surgeons actually embark on right hemicolectomy for appendiceal mass as soon as the patients present.2,5,8 Immediate appendectomy has the advantages of being safe, eliminates risk of recurrent appendicitis and eliminates the need for re-admission for interval appendectomy.5 It is generally reported to reduce total hospital stay2,8 However, it has a high complication rate of about 36%, almost comparable to that for perforated appendicitis.9 Immediate surgery leads to dissemination of infection and intestinal fistula formation.2 This obviously seems to obviate the advantages enumerated above. The inflammatory appendiceal mass may be mistaken at surgery for a malignant tumor, occasionally leading to right hemicolectomy. A malignant mass may be mistakenly under-treated by appendectomy. In view of the above complications it is advisable not to adopt this method in our environment, as this group has significant complications and over treatment compared to the traditional initial conservative method. Approach C An entirely conservative approach without interval appendicectomy in patients with appendiceal mass A school of thought argued that after a successful conservative management, interval appendicectomy is not necessary and can safely be omitted, except in patients with recurrent symptoms. In patients above 40 years of age, one must exclude other pathological causes of right iliac fossa mass by further investigations such as barium enema, colonoscopy and computerized tomography scan. A close follow up is needed in this category of patients.18 Obviously patients in Groups A and B above have significantly longer duration of hospital stay as well as time lost from work. Dixon et al20 reviewed the characteristics of 32 patients who had recurrence of symptoms following conservative managemen.t20 Mean time to recurrence was five months following the initial episode. They compared the clinical characteristics of each patient at initial admission with the same characteristics at recurrence. They demonstrated that when recurrence of appendicitis occurs this followed a milder clinical course. The recurrences were treated successfully with both operative and non-operative approaches and were not associated with any significant mortality or morbidity. They also compared clinical and demographic characteristics of the recurrence group to the non-recurrence group and found no significant risk factors for recurrence, including the severity of the initial presentation. There is, therefore, good evidence, first, that the risk of recurrent acute appendicitis following successful conservative management is low; between 5% and 14%. Second, in the minority of patients whose symptoms do recur, this usually occurs within one year. Third, recurrence of appendicitis following conservative management is usually associated with a milder clinical course amenable to both operative and non-operative approaches. Fourthly, there is no accurate method for predicting patients at risk of recurrence. The conservatively managed group also had the shortest length of hospital stay even when the recurrences were included. They concluded that conservative management without interval appendicectomy was the most appropriate management for appendix mass and that immediate appendicectomy should only be used when initial conservative management fails.21,23,25,29 Conclusion Misdiagnosis of appendiceal tumor or colonic tumor can be disastrous in patients with appendiceal mass so we should exercise caution when adopting entirely conservative approach. Sophisticated investigations such as MRI, CT scans are not easily accessible in this part of the world. Hence to adequately rule out other pathologies may be difficult when we adopt entirely conservative approach. A traditional initial conservative management is still a highly acceptable approach for appendix mass. This should be followed with interval appendicectomy more so in patients with persistent right lower abdominal pain. During the waiting period further investigating should be carried out. Advanced imaging techniques should not be applied routinely although they may be valuable when the clinical diagnosis is uncertain. Ultrasound is particularly valuable in women. Active observation is an appropriate method for managing uncertain cases. References
Copyright 2008 - Annals of African Medicine The following images related to this document are available:Photo images[am08041f1.jpg] |
| |||||||||

{kind=link}