 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
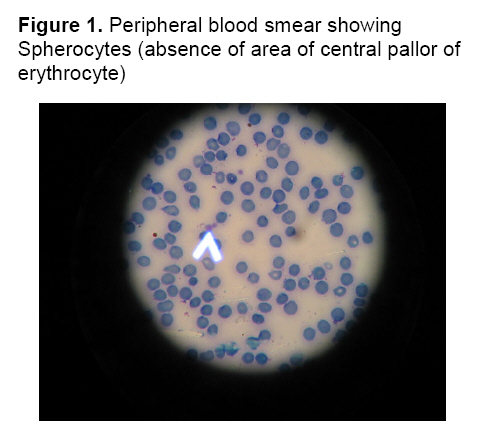
Annals of African Medicine, Vol. 8, No. 1, March, 2009, pp. 61 - 63 Hereditary Spherocytosis in a 27-Year-old Woman: Case Report A.Hassan, A. A.Babadoko, A. H.Isa and P.Abunimye Departments
of Haematology, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria Accepted: 14th August 2008 Code Number: am09013 Abstract Hereditary spherocytosis (HS) is a familial hemolytic disorder with marked heterogeneity of clinical features, ranging from an asymptomatic condition to a fulminant hemolytic anemia. Although a positive family history of spherocytosis increases the risk for this disorder, it may be sporadic in some cases. In severe cases the disorder may be detected in early childhood, but in mild cases it may go unnoticed until later in adult life. A 27-year-old Nigerian woman presented with mild anemia, jaundice, splenomegaly and a history of multiple blood transfusion. Blood film showed about 70% spherocytes, reticulocytosis of 6.5%, increased osmotic fragility test and a negative direct antiglobulin test. She was managed conservatively on nutritional supplements and a significant regression of symptoms after 6 months was achieved. Keywords: Anaemia, jaundice, splenomegaly, hereditary, spherocytosis Résumé Le spherocytosis héréditaire (HS) est un désordre hémolytique familial avec l'hétérogénéité marquée des dispositifs cliniques, s'étendant d'un état asymptomatique à une anémie hémolytique fulminante. Bien que des antécédents familiaux positifs de spherocytosis augmentent le risque pour ce désordre, ils peuvent être sporadiques dans quelques cas. Dans des cas graves le désordre peut être détecté dans l'enfance tôt, mais dans des cas doux il peut entrer inaperçu jusque postérieur à la vie d'adulte. Une femme nigérienne de 27 ans s'est présentée avec l'anémie douce, l'ictère, le splenomegaly et une histoire de transfusion sanguine multiple. Le film de sang a montré les spherocytes environ de 70%, reticulocytosis de 6.5%, a augmenté l'essai osmotique de fragilité et un essai direct négatif d'antiglobulin. Elle a été contrôlée conservativement sur des suppléments alimentaires et une régression significative des symptômes après 6 mois a été réalisée. Mots-clés: Anémie, ictère, splenomegaly, héréditaire, spherocytosis Hereditary spherocytosis (HS) is a rare inherited red blood cell membrane disorder that is characterized by spherically shaped red blood corpuscles on peripheral blood smear.1-3 Hereditary spherocytosis was described initially in 1871.4 It is the most common inherited hemolytic anemia in Caucasians with an incidence of 1: 2500-5000 population.2,3 It also occurs in people of African and Mediterranean descent accounting for 1: 2000 of the population.3 Most cases are inherited in an autosomal dominant fashion.4 Approximately 25% of cases are discovered in persons who have no family history of HS; these cases may represent spontaneous mutations or recessive forms of the disease.4 Calculations indicate that the HS silent carrier state might exist in 1.4% of the population.4 This case is reported in view of the rarity of this disorder coupled with the few specialists (Haematologist) to diagnose and manage such a disorder in our environment. It is hoped that this report will bring increase awareness on the existence of HS in our environment and hence an increase index of suspicion and prompt referral to avoid unnecessary use of blood transfusion. Case report A 27-year-old woman presented with recurrent abdominal swelling, stunted growth relatively to her siblings and age groups. She has had four units of blood transfusion in childhood; her last transfusion was 10 years prior to presentation. She also has recurrent yellowish discoloration of the eyes. No family history of sickle cell disease. Examination revealed a young lady, with a small and short stature, mildly pale, moderately jaundiced and has a gnathopathy. The spleen was enlarged by 6cm below the right costal margin but the liver was not palpably enlarged. Laboratory investigation shows a haematocrit of 0.27 (Hb 9g/dL), white blood cell count of 6.2x109/L, platelet count of 201x109/L, MCV of 75µm3 (80-97) reduced, MCHC of 37g/dl (31.5-35) increased. Peripheral blood smear showed a predominance of spherocytes constituting over 70% of the red blood cells (Figure 1). The white cell and platelets are of normal morphology. Her genotype was AA. A high reticulocytes count of 6.5% was obtained. A direct antiglobulin test was then performed which was negative but the osmotic fragility test was increased. The diagnosis of hereditary spherocytosis was then made and the patient was counseled and placed on folic acid supplementation and a three monthly follow up visit. After six months, her clinical state improved with jaundice decreasing to just a tinge, the spleen regressed to 2cm while the packed cell volume increased to 0.30 (Hb 10 g/dL). Discussion Hereditary Spherocytosis is the commonest inherited red cell membrane disorder. It is generally a rare disease world wide.1-3 This is confirmed by this report of one case over a period of fifteen years in Ahmadu Bello University Teaching Hospital, Zaria, although this patient was a youth corp member from the eastern part of Nigeria, who was posted to the Northern part of the country. Oluboyede et al in 1976 reported five cases at University college hospital, Ibadan.9 The incidence and prevalence in other ethnic groups in Nigeria have not been clearly established as reported by Oluboyede et al but he proposed that since the cases came from widely separated area, no ethnic group has more predilection than others.9 Hereditary Spherocytosis results from primary red cell membrane cytoskeleton defect.3 Spectrin deficiency is the most common defect. The defects are associated with a variety of mutations that result in different protein abnormalities and varied clinical expression. Most cases of HS are heterozygous because homozygous states are lethal.1-4 In pedigrees that have a dominant defect, affected family members tend to have similar degrees of hemolysis and clinical severity.5-7 Regardless of the molecular basis for a case of HS, the resulting spherocytes become trapped in the spleen as they course through the sinuses, and the red cells are engulfed by macrophages.5-7 Several reports and text books have associated a triad of anemia, jaundice and splenomegaly to the morphological findings of spherocytes as the hallmark to the diagnosis of HS as was the finding in this case.1,2,4,6 Our diagnosis was supported by an increased osmotic fragility and a negative direct comb’s test, although a negative result may be obtained especially for osmotic fragility where a high reticulocytes count of more than 10% interferes with the test.4 The clinical presentation of this patient is similar to those cases reported at Ibadan and other parts of the World.1,2,4,6,8 In the first few postnatal months, anemia can develop in children who do not mount an adequate reticulocyte response.4 In later childhood, HS can present with anemia, jaundice, and splenomegaly.4-6 Affected patients may have mild, moderate, or severe anemia. Children who have moderate-to-severe anemia may have poor exercise tolerance, poor growth, and academic difficulties.4-6 Older individuals develop bilirubin stones and may present with cholecystitis.4-6 It is often not uncommon for the diagnosis to be missed until adult hood. The peripheral blood smear in HS shows numerous spherocytes. Larger bluish cells (polychromasia) also may be seen. The complete blood count (CBC) and reticulocyte count reveal a low hemoglobin concentration and elevated reticulocyte count.1-3 The mean corpuscular hemoglobin concentration is usually high at greater than 35 g/dL (350 g/L). The mean corpuscular volume may be low or high if there is substantial reticulocytosis.1-3 The test of osmotic fragility can be useful in establishing the diagnosis of HS. Spherocytes have reduced cell membranes and thus they swell at higher concentrations of saline than do normal red cells. The direct antiglobulin (coombs) test is usually negative. Other test include elevated unconjugated bilirubin, elevated lactic dehydrogenase, and low haptoglobin levels. However, these findings are associated with any case of haemolysis and are not specific for HS.1-3 A family study could not be carried in this case since her family resides in the Eastern part of the country. However she denied any member of the family with neither a similar history nor physique. Thus this may be recessively inherited or sporadic as it occurs in 25% of cases or a silent carrier state, as it has been suggested to exist in 1.4% of the population.4 The patient was managed conservatively with nutritional supplementation consisting of folic acid, ascorbic acid and paludrine for prophylaxis against malaria. The red cell transfusion she had before Haematologist review may have been avoided if a definitive diagnosis was made and appropriate therapy instituted and the effect on growth pattern and the risk of allogeneic blood transfusion would have been limited. Specific indications for transfusion include exacerbation of anemia due to blood loss such as related to trauma or surgery, hypersplenism, and infection with parvovirus B19.4 Cure is achieved with splenectomy4 but there was no indication for this in our patient. Splenectomy is carried out in cases with severe anemia and extramedullary hematopoiesis.4 Complications of hereditary spherocytosis include pigment gallstones, aplastic, haemolytic and megaloblastic crises, poor growth, skeletal deformities, and less commonly skin ulceration, chronic dermatitis.1-3 Although HS is rare it does occur in our environment and when suspected hematological assessment is necessary to avoid diagnostic pitfalls and mismanagement. References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09013f1.jpg] |
| |||||||||

{kind=link}