 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
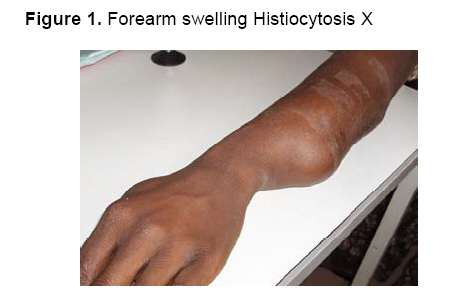
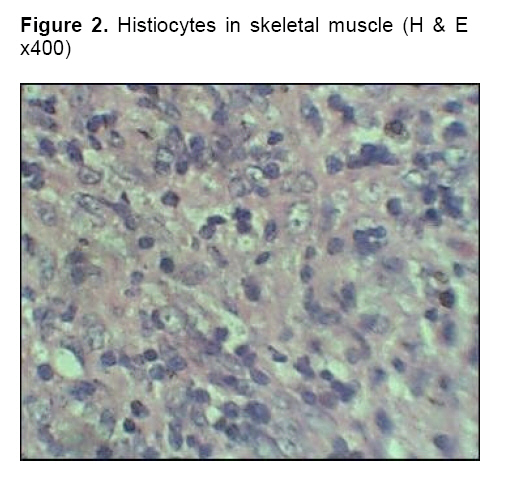
Annals of African Medicine, Vol. 8, No. 1, March, 2009, pp. 64 - 65 Histiocytosis X 1A.Mohammed, 2L. Z.Yau, 1M.O.A.Samaila, 1S. A.Ahmed and 3N. D.Chom 1Departments of Pathology, Ahmadu Bello University Teaching Hospital, Shika, Zaria, Nigeria Accepted: 13th August 2008 Code Number: am09014 Histiocytosis X (Langerhan’s cell granulomatosis) is a disease of unknown aetiology, but viral origin has been implicated.1 It is a clinicopathologic entity characterized by proliferation of Langerhan’s cell (which are not primarily phagocytic) in an appropriate milieu.2 A 27-year-old man presented with a 6-year history of painless progressive left forearm swelling. There was no antecedent history of trauma or surgical maneuvers. His past medical history was insignificant. Clinical examination revealed a well preserved young man with a non-tender globular doughy left forearm swelling to the wrist level measuring 16×18cm and stretched overlying skin with prominent veins (Figure 1). The radial artery pulsation was good. Skin sensation was also preserved. Radiograph of the forearm (Figure 2) showed lytic destruction of the ulnar bone and soft tissue swelling. He had a packed cell volume of 37%. Other blood parameters and chemistry were normal. Tissue biopsy and histology showed diffuse sheets of histiocytes having cleft nuclei and granular eosinophilic cytoplasm invading into the skeletal muscle and necrotic bone trabeculae (Figure 3). It was diagnosed Histiocytosis X. Ablative surgery was declined by the patient. Histiocytosis X has been grouped into many clinical types (Table1) which overlap depending on the age, organ (s) affectation and number of lesions in any particular organ. It may present as a solitary lesion or with multiple foci in an organ or as a systemic disease with many organ affectation.3 Several organs such as skin, bone, female genital tract, lymph node, lung, thymus, stomach and central nervous system have been implicated.4 The commonest site is the bone.5 Pathologic staging of the disease is divided into four groups (Table2). Osteolytic lesions are uncommon except in the mastoid region of the temporal bone.6 Table 1. Simplified approach to types of histiocytosis1
Table2. Pathologic staging of langerhan’s cell diseases
Definitive diagnosis of Histiocytosis X was based on electron microscopic identification of Birbeck’s cell or langerhan’s granule, which are elongated zipper like cytoplasmic structures of indeterminate fuction.2 Diagnosis is also possible with light microscopic examination of paraffin embedded tissue as in this case, by the identification of mononuclear cells (histiocytes) characterized by irregular, elongated nuclei with prominent nuclear grooving and folds and an eosinophilic cytoplasm.1 Immunohistochemical identification of S – 100 and CD1a antigen is also helpful.1 Generally, this disease runs a benign course. In its mildest form it is an eosinophilic granuloma and may require only a biopsy for confirmation. Lesions which are shown to invade surrounding skeletal muscles exhibit the worst in terms of outcome and are shown to cause multiple organ dysfunction.7 Other modalities of treatment for less aggressive form of the disease include: curettage and bone grafting, radiotherapy and corticosteroids with varying degrees of success.8 References
Copyright 2009 - Annals of African Medicine The following images related to this document are available:Photo images[am09014f3.jpg] [am09014f2.jpg] [am09014f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}